I have sat across from hundreds of women in my clinic in Gomti Nagar who received the same diagnosis and walked away with the same hollow feeling: blocked fallopian tubes. Some had been told by well-meaning relatives that they would never conceive. Some had spent months on treatments that were never going to work for their specific condition. A few had quietly convinced themselves that motherhood simply was not meant for them.
I want to say this clearly, from two decades of clinical experience:
A diagnosis of blocked fallopian tubes is not the end of your parenthood journey. It is the beginning of a very clear path forward. That path is IVF.
IVF for tubal block is not a last resort. It is the most logical, most effective, and in most cases, the most direct solution available. Here is everything you need to understand about your diagnosis and your options.
What Is Tubal Block, and Why Does It Prevent Natural Pregnancy?
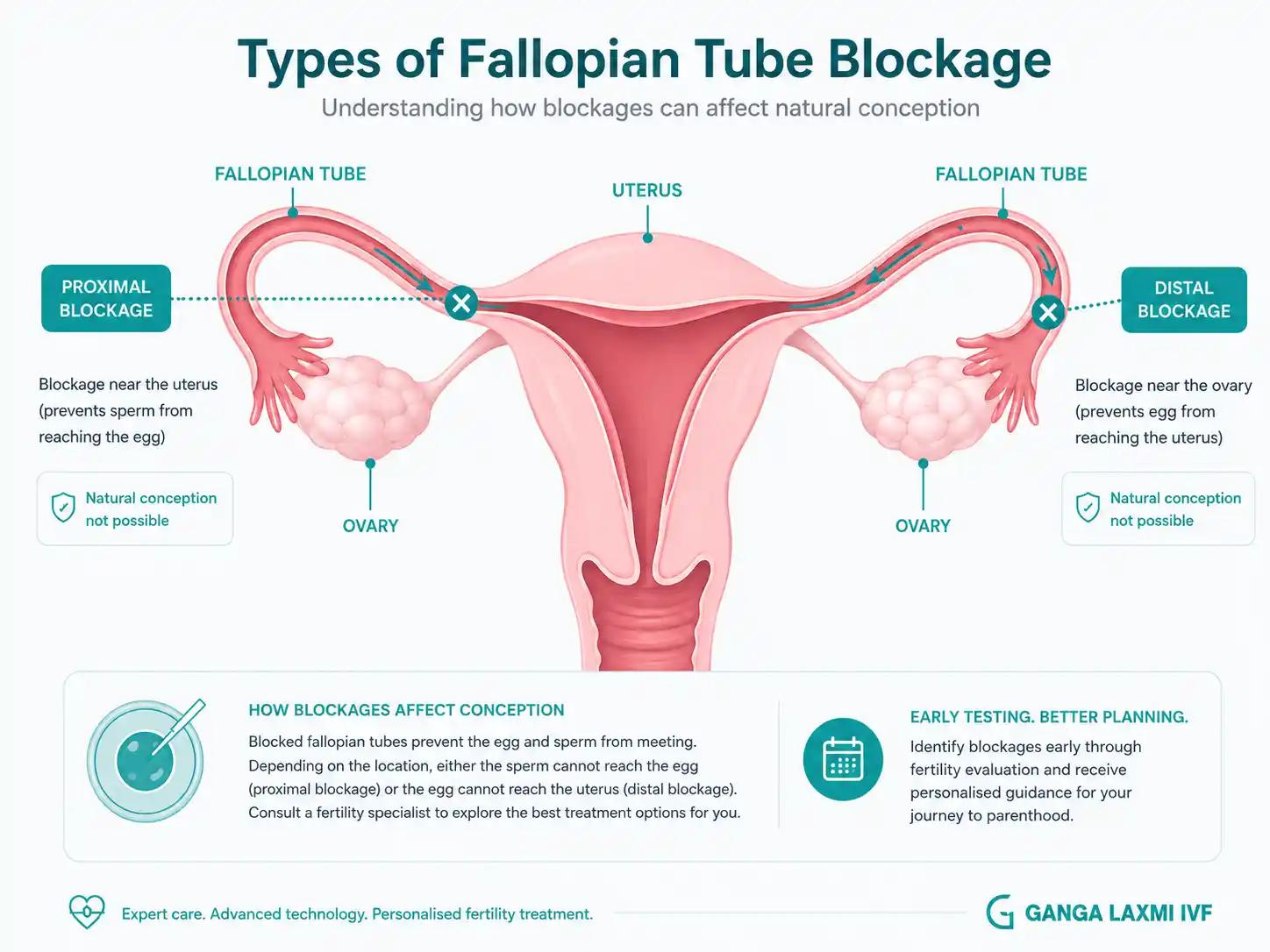
Your fallopian tubes are the bridge between your ovaries and your uterus. Every month, when an egg is released, it travels through this tube. Sperm swim up through the uterus into the tube to meet the egg there. Fertilisation happens inside the tube, not the uterus. The resulting embryo then travels down the tube over the next few days and implants in the uterine wall.
When one or both tubes are blocked, this journey cannot happen. The egg and sperm either never meet, or the embryo has no route to the uterus.
The Three Types of Tubal Blockage
Proximal Blockage
What It Means
Occurs near the junction where the tube meets the uterus. Sometimes caused by mucus plugs, spasms, or scarring. Occasionally addressable with selective procedures, though results vary.
Distal Blockage
What It Means
Affects the far end of the tube, closest to the ovary. Often associated with hydrosalpinx, where the blocked tube fills with fluid that can be toxic to embryos.
Bilateral Blockage
What It Means
Both tubes affected. Natural pregnancy and most other fertility treatments are not possible. IVF is the definitive treatment.
| Type | What It Means |
|---|---|
| Proximal Blockage | Occurs near the junction where the tube meets the uterus. Sometimes caused by mucus plugs, spasms, or scarring. Occasionally addressable with selective procedures, though results vary. |
| Distal Blockage | Affects the far end of the tube, closest to the ovary. Often associated with hydrosalpinx, where the blocked tube fills with fluid that can be toxic to embryos. |
| Bilateral Blockage | Both tubes affected. Natural pregnancy and most other fertility treatments are not possible. IVF is the definitive treatment. |
Common Causes: Notes for Lucknow and UP Patients
Tubal block is not anyone's fault. It is a structural outcome of events, many of them invisible , that happened to your body. Understanding the cause helps us plan treatment, but there is no place for guilt in this conversation.
Pelvic Inflammatory Disease (PID)
Notes for UP / Lucknow Patients
Most common cause. Recurrent or undertreated infections lead to tubal scarring.
Genital Tuberculosis (TB)
Notes for UP / Lucknow Patients
Significant and under-recognised in Uttar Pradesh. Many patients have no obvious TB history yet show tubal damage on investigation.
Endometriosis
Notes for UP / Lucknow Patients
Uterine-like tissue growing outside the uterus causes adhesions and scarring around the tubes.
Prior Pelvic Surgery
Notes for UP / Lucknow Patients
Appendectomy, C-section, fibroid removal, any pelvic procedure can cause adhesions.
STIs (e.g. Chlamydia)
Notes for UP / Lucknow Patients
Can damage tubes silently over years with no noticeable symptoms.
Ectopic Pregnancy
Notes for UP / Lucknow Patients
Affects or removes the involved tube permanently.
| Cause | Notes for UP / Lucknow Patients |
|---|---|
| Pelvic Inflammatory Disease (PID) | Most common cause. Recurrent or undertreated infections lead to tubal scarring. |
| Genital Tuberculosis (TB) | Significant and under-recognised in Uttar Pradesh. Many patients have no obvious TB history yet show tubal damage on investigation. |
| Endometriosis | Uterine-like tissue growing outside the uterus causes adhesions and scarring around the tubes. |
| Prior Pelvic Surgery | Appendectomy, C-section, fibroid removal, any pelvic procedure can cause adhesions. |
| STIs (e.g. Chlamydia) | Can damage tubes silently over years with no noticeable symptoms. |
| Ectopic Pregnancy | Affects or removes the involved tube permanently. |
How Is Tubal Block Diagnosed? My Diagnostic Approach
Correct diagnosis is everything. I have seen patients referred to me after being told they have bilateral tubal block, and on proper evaluation, the picture was entirely different. Diagnosis must be thorough and precise.
HSG (Hysterosalpingography)
What It Shows
Dye injected through cervix; X-ray shows whether tubes are open. First-line investigation.
Dr. Chauhan's Note
Can produce false positives due to tubal spasm. Never make a final decision on HSG alone.
Diagnostic Laparoscopy
What It Shows
Direct visualisation of tubes, pelvic anatomy, adhesions, and endometriosis.
Dr. Chauhan's Note
Gold standard. Dr. Chauhan performs this herself, same doctor evaluates and treats, no handover.
Saline Sonography (SIS / HyCoSy)
What It Shows
Ultrasound-based assessment of tubal patency.
Dr. Chauhan's Note
Useful as a gentler screening option in selected cases.
| Investigation | What It Shows | Dr. Chauhan's Note |
|---|---|---|
| HSG (Hysterosalpingography) | Dye injected through cervix; X-ray shows whether tubes are open. First-line investigation. | Can produce false positives due to tubal spasm. Never make a final decision on HSG alone. |
| Diagnostic Laparoscopy | Direct visualisation of tubes, pelvic anatomy, adhesions, and endometriosis. | Gold standard. Dr. Chauhan performs this herself, same doctor evaluates and treats, no handover. |
| Saline Sonography (SIS / HyCoSy) | Ultrasound-based assessment of tubal patency. | Useful as a gentler screening option in selected cases. |
Dr. Chauhan's Diagnostic Pathway
Begin with HSG. Confirm with laparoscopy when indicated. Correlate with your full clinical history and, where relevant in UP, a TB workup. The same specialist who evaluates you will plan and conduct your IVF , with no reports handed between doctors.
Why IVF Is the Best Solution for Tubal Block
This is the question that changes everything for most of my patients, and the answer is remarkably straightforward.
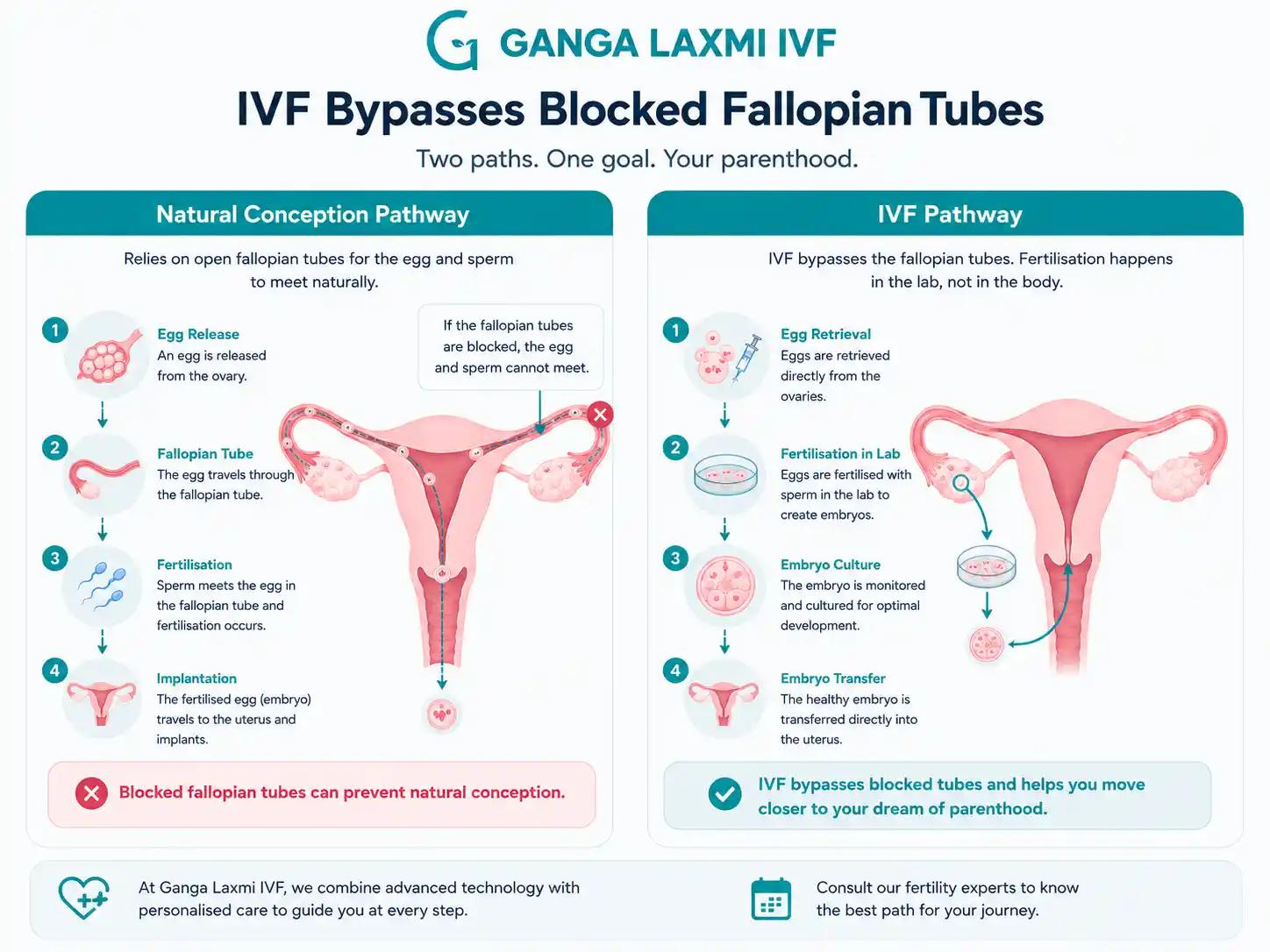
IVF completely bypasses the fallopian tubes at every single step.
In a natural conception, the tubes are indispensable. In an IVF cycle, they play absolutely no role. Here is what happens instead:
- Your ovaries are stimulated with carefully titrated hormonal injections to produce multiple mature eggs.
- Eggs are retrieved directly from your ovaries through a minor ultrasound-guided procedure, with no tubes involved involved.
- The eggs are fertilised with sperm in our embryology lab and cultured for 3 to 5 days.
- The healthiest embryo is placed directly into your uterus through your cervix using a fine catheter.
The tubes are not consulted, passed through, or required at any point. Whether both your tubes are blocked, damaged, filled with fluid, or surgically absent, it makes no difference to the IVF process. This is why IVF for tubal block produces success rates comparable to IVF for any other diagnosis. The tubes were the only broken link in the chain. IVF removes that link entirely.
Note on Hydrosalpinx
If investigations reveal hydrosalpinx (fluid-filled tubes), laparoscopic removal or clipping of the affected tube is typically recommended before embryo transfer. Research consistently shows this improves IVF success rates by preventing toxic fluid from entering the uterine cavity. Dr. Chauhan performs this procedure herself and will discuss it with you during planning.
Can Tubal Block Be Treated Surgically? An Honest Assessment
Patients frequently ask me this, and I appreciate the question, because it tells me they are thinking carefully about their options rather than simply accepting the first recommendation they receive.
Tubal surgery (tuboplasty) is technically possible in select cases. However, results are limited and unpredictable for reasons that matter clinically.
Success Rate
Tubal Surgery
Unpredictable; limited by cilia damage
IVF
Comparable to IVF for other diagnoses
Tubes Required
Tubal Surgery
Yes, if the tube is functional
IVF
No, tubes are bypassed entirely
Recovery Time
Tubal Surgery
4 to 6 weeks post-surgery before trying
IVF
Begin IVF immediately after healing
Risk of Ectopic
Tubal Surgery
Higher if the repaired tube does not function
IVF
Lower, embryo placed directly in the uterus
Best For
Tubal Surgery
Mild proximal block, young patient, no other factors
IVF
Bilateral block, TB damage, hydrosalpinx, moderate-severe disease
Dr. Chauhan's Approach
Tubal Surgery
Assessed via direct laparoscopic evaluation
IVF
Default recommendation for most tubal cases
| Factor | Tubal Surgery | IVF |
|---|---|---|
| Success Rate | Unpredictable; limited by cilia damage | Comparable to IVF for other diagnoses |
| Tubes Required | Yes, if the tube is functional | No, tubes are bypassed entirely |
| Recovery Time | 4 to 6 weeks post-surgery before trying | Begin IVF immediately after healing |
| Risk of Ectopic | Higher if the repaired tube does not function | Lower, embryo placed directly in the uterus |
| Best For | Mild proximal block, young patient, no other factors | Bilateral block, TB damage, hydrosalpinx, moderate-severe disease |
| Dr. Chauhan's Approach | Assessed via direct laparoscopic evaluation | Default recommendation for most tubal cases |
For patients with bilateral blockage, tuberculosis-related damage, or moderate-to-severe disease, surgical repair rarely offers a realistic path to pregnancy and simply delays the start of effective treatment.
I perform laparoscopic surgery myself at Ganga Laxmi IVF, which means I evaluate tubal anatomy directly and can have an honest, personalised conversation with you about whether surgery could add value in your specific case, or whether proceeding directly to IVF gives you the best chance in the shortest time.
IVF for Tubal Block at Ganga Laxmi IVF, Lucknow
When a patient comes to me with tubal block, I do not give her a standard protocol. I give her my full clinical attention.
Before starting any IVF cycle, I take a complete history, review all prior investigations, and personally assess the uterus, tubes, and ovarian reserve. If there is any suspicion of genital TB, which is far more common in UP than most centres acknowledge, I complete a full TB workup and ensure treatment is completed before embryo transfer.
What Distinguishes Care at Ganga Laxmi IVF
Single specialist continuity
Why It Matters
You see Dr. Kumudini Chauhan at every key appointment, not a rotating junior doctor. Tubal block patients often have complex histories that require consistent clinical judgement.
Personal TB workup when indicated
Why It Matters
Genital TB is a significant, under-diagnosed cause of tubal block in UP. Treating it before embryo transfer is essential and often overlooked at other clinics.
Laparoscopic expertise in-house
Why It Matters
The doctor who evaluates your tubes is the same doctor who will perform your IVF. No second-hand reports, no gaps in clinical understanding.
Individualised stimulation protocols
Why It Matters
Protocol adjusted for your age, ovarian reserve, prior cycle response, and specific cause of blockage, not a default template.
Hydrosalpinx management before transfer
Why It Matters
Where indicated, Dr. Chauhan manages hydrosalpinx laparoscopically before embryo transfer, following evidence-based best practice.
| What We Do | Why It Matters |
|---|---|
| Single specialist continuity | You see Dr. Kumudini Chauhan at every key appointment, not a rotating junior doctor. Tubal block patients often have complex histories that require consistent clinical judgement. |
| Personal TB workup when indicated | Genital TB is a significant, under-diagnosed cause of tubal block in UP. Treating it before embryo transfer is essential and often overlooked at other clinics. |
| Laparoscopic expertise in-house | The doctor who evaluates your tubes is the same doctor who will perform your IVF. No second-hand reports, no gaps in clinical understanding. |
| Individualised stimulation protocols | Protocol adjusted for your age, ovarian reserve, prior cycle response, and specific cause of blockage, not a default template. |
| Hydrosalpinx management before transfer | Where indicated, Dr. Chauhan manages hydrosalpinx laparoscopically before embryo transfer, following evidence-based best practice. |

What to Expect: Your IVF Journey with Tubal Block, Step by Step
Understanding each step before you begin makes the process feel less daunting and more manageable. Here is exactly what your journey looks like at Ganga Laxmi IVF.
Consultation and Diagnosis Confirmation
Detailed history, review of all prior reports, baseline ultrasound, and hormonal assessment. Where tubal diagnosis requires confirmation, we plan the appropriate investigation at this stage.
Personalised Protocol Planning
Dr. Chauhan designs your ovarian stimulation protocol based on your investigations. Timeline, injections, monitoring schedule, and all questions answered before starting.
Ovarian Stimulation
Daily hormonal injections for approximately 10 to 12 days stimulate multiple mature eggs. Monitoring ultrasounds throughout. Dr. Chauhan adjusts doses in real time based on your response.
Egg Retrieval
A minor procedure under sedation, completed in under 30 minutes. Eggs retrieved directly from ovaries using a fine ultrasound-guided needle. You go home the same day.
Fertilisation and Embryo Culture
Eggs fertilised in the embryology lab with standard IVF or ICSI as indicated. Embryos cultured for 3 to 5 days with daily development updates.
Embryo Transfer
The healthiest embryo placed directly into the uterus. A simple, painless procedure with no anaesthesia required. Return home shortly after.
Pregnancy Test
A blood test for beta-hCG approximately 14 days after transfer. Dr. Chauhan ensures you are not navigating this moment alone.
Help centre
Frequently Asked Questions
These are questions I hear every week in my clinic, questions patients often hesitate to ask, but absolutely should.
Yes, it is biologically possible. Some women with one healthy tube do conceive naturally, particularly if the blockage is mild and there are no other fertility factors. However, natural conception with one blocked tube takes significantly longer on average, and the risk of ectopic pregnancy in the remaining tube is elevated. If you have been trying for 6 to 12 months without success, or if you are over 35, I recommend a fertility evaluation rather than continuing to wait. Time is a real factor in fertility.
IVF is as safe for tubal block patients as it is for any other diagnosis. The tubes play no role in the IVF process, so their condition does not add any procedural risk. The one exception worth knowing: if you have hydrosalpinx, laparoscopic treatment of the affected tube before embryo transfer is recommended. The fluid from a hydrosalpinx can enter the uterine cavity and significantly reduce implantation rates. Addressing it first protects your IVF cycle and improves your chances.
There is no single honest answer without knowing your full picture. Tubal block by itself does not reduce IVF success rates. Your chances are comparable to someone doing IVF for other reasons. Success per cycle typically ranges from 40 to 60% for women under 35 with good ovarian reserve, declining with age. Many patients with tubal block conceive in their first cycle. I recommend planning emotionally and financially for up to three cycles while genuinely hoping for success in the first cycle. This balance of optimism and preparedness makes the journey more sustainable.
The answer depends entirely on the nature of your blockage. For mild proximal blockage in a young patient with no other complicating factors, a discussion about surgical correction is worth having. For bilateral damage, extensive scarring, hydrosalpinx, or TB-related damage, which represent the majority of cases I see in Lucknow, proceeding directly to IVF gives a far better chance of pregnancy and avoids an unnecessary surgical recovery period. I will assess your specific anatomy and give you an honest, direct recommendation.
Tubal factor infertility actually has some of the best IVF outcomes among all infertility diagnoses, because the tubes are the only problem. Once we bypass them, the rest of the system often works well. Success rates are primarily determined by the woman's age, ovarian reserve, embryo quality, and uterine health, all of which I review with every patient before predicting outcomes for their specific situation. Tubal block is one of the diagnoses I am most confident treating, because IVF is a complete solution, not a workaround.
You Have More Options Than You Were Told
A diagnosis of blocked fallopian tubes is not a closed door. For thousands of families treated in Lucknow and across Uttar Pradesh, it was the moment that finally led them to the right treatment.
If you have been told your tubes are blocked, if you have been trying to conceive without success, or if you simply want to understand your options clearly and honestly. I would like to meet you.
Ready to take the next step?
Book a consultation with Dr. Kumudini Chauhan
Tubal block, hydrosalpinx, or TB-related damage. Meet the specialist who will guide your IVF journey from first visit to pregnancy test at Ganga Laxmi IVF, Gomti Nagar.
- Clinic
- 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow, 226010
- Hours
- Monday to Saturday, 9:00 AM to 8:00 PM
- Phone
- +91 72756 49692
- First consultation
- From Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
Tubal factor IVF
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles
Male Infertility Treatment in Lucknow: Causes, Tests & Complete Guide
Male factors contribute to roughly half of all infertility cases. Dr. Kumudini Chauhan explains what causes male infertility, what a proper investigation looks like, and which treatments, from lifestyle changes to ICSI, are available at Ganga Laxmi IVF, Lucknow.

Laser Hatching and PGT After Failed IVF: Why Your Previous Cycles Failed and What to Do Next
Dr. Kumudini Chauhan explains why IVF fails, how Laser Assisted Hatching and PGT address those specific causes, and what a proper failed-IVF workup looks like at Ganga Laxmi IVF.

IVF After 40 in Lucknow: Advanced Age Fertility, PGT, and Realistic Hope
Fewer eggs, more chromosomal errors, harder decisions. Dr. Kumudini Chauhan explains what age actually does to your fertility, how PGT changes the odds, and what advanced age IVF looks like at Ganga Laxmi IVF, Lucknow.
PCOS and Pregnancy: Can You Conceive with PCOS?
Irregular cycles, no ovulation, conflicting advice. Dr. Kumudini Chauhan explains what PCOS actually does to your fertility, which treatments work at each stage, and what to expect at Ganga Laxmi IVF, Lucknow.