The first time a nurse tells you that you can hold your premature baby against your chest, really hold them, skin to skin, not just through the glass of an incubator, something shifts.
For many parents, that moment is the first time they feel like a parent rather than a bystander. It is also the beginning of one of the most medically significant things you can do for your baby's survival and development.
That moment has a name: Kangaroo Mother Care.
This article explains what KMC is, what it does for your baby and for you, which babies are eligible, how to do it safely, and what current international guidelines say about when to start. Everything here is grounded in WHO evidence. Confirm all clinical guidance with your care team before you begin.
1. What Is Kangaroo Mother Care?
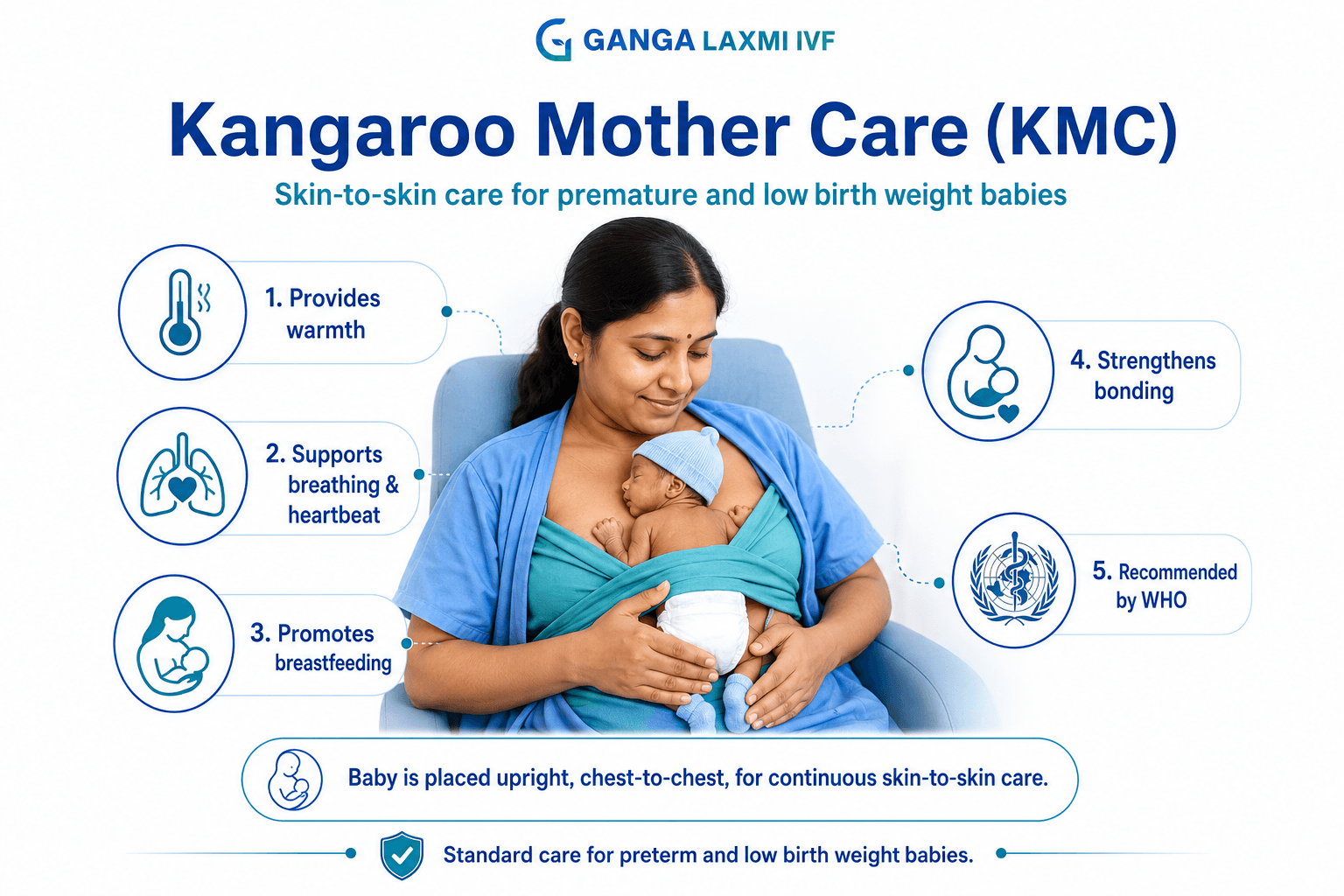
Kangaroo Mother Care (KMC) is a method of caring for premature and low birth weight babies through continuous skin to skin contact with a parent or caregiver. The baby is placed upright, directly against the parent's bare chest, between the breasts, wearing only a diaper, cap, and socks. The caregiver's body provides warmth, heartbeat, breathing rhythm, and proximity that the baby's own systems are not yet mature enough to maintain independently.
The method was developed in Bogota, Colombia in 1978 by Doctors Edgar Rey and Hector Martinez, after a shortage of incubators forced them to find an alternative. Babies cared for this way survived at rates comparable to incubator care, and in some measures better. The name comes from how kangaroo joeys continue developing in their mother's pouch, a comparison that captures exactly what the technique achieves.
WHO now recommends KMC as the essential standard of care for all preterm and low birth weight babies, starting right after birth. It is endorsed by WHO, UNICEF, the American Academy of Pediatrics, and the Indian Academy of Pediatrics. See the WHO KMC guidelines for full detail.
2. KMC vs Incubator Care: A Comparison
Many parents wonder whether holding their baby is truly as effective as the incubator. The answer, backed by WHO evidence, is that KMC is not an alternative to good medical care, it is an essential part of it.
Warmth
Kangaroo Mother Care
Dynamic, parent's body adjusts in real time
Incubator Care
Static, fixed setting, no automatic response
Breastfeeding
Kangaroo Mother Care
Strongly supported, proximity triggers let-down and feeding cues
Incubator Care
Not supported during incubator time
Bonding
Kangaroo Mother Care
Direct and continuous
Incubator Care
Limited to handling through portholes
Infection risk
Kangaroo Mother Care
Maternal skin flora builds baby's microbiome; reduces sepsis risk
Incubator Care
No microbiome benefit; risk of hospital-acquired organisms
Baby's stress
Kangaroo Mother Care
Lower cortisol, stable heart rate, longer deep sleep
Incubator Care
Higher sensory stress from alarms and handling
Parent mental health
Kangaroo Mother Care
25% lower risk of moderate-severe maternal depression
Incubator Care
Separation increases anxiety and depression risk
Cost
Kangaroo Mother Care
Free, no equipment needed
Incubator Care
Requires expensive equipment and maintenance
WHO recommendation
Kangaroo Mother Care
Standard of care for all preterm/low birth weight babies from birth
Incubator Care
Used for unstable babies needing respiratory/cardiac support
| Feature | Kangaroo Mother Care | Incubator Care |
|---|---|---|
| Warmth | Dynamic, parent's body adjusts in real time | Static, fixed setting, no automatic response |
| Breastfeeding | Strongly supported, proximity triggers let-down and feeding cues | Not supported during incubator time |
| Bonding | Direct and continuous | Limited to handling through portholes |
| Infection risk | Maternal skin flora builds baby's microbiome; reduces sepsis risk | No microbiome benefit; risk of hospital-acquired organisms |
| Baby's stress | Lower cortisol, stable heart rate, longer deep sleep | Higher sensory stress from alarms and handling |
| Parent mental health | 25% lower risk of moderate-severe maternal depression | Separation increases anxiety and depression risk |
| Cost | Free, no equipment needed | Requires expensive equipment and maintenance |
| WHO recommendation | Standard of care for all preterm/low birth weight babies from birth | Used for unstable babies needing respiratory/cardiac support |
Clinical position: Unstable babies who need active respiratory or circulatory support require NICU equipment. Once stable, KMC is not a downgrade from incubator care, it is the superior standard of care for most outcomes that matter.
3. WHO Key Statistics on Kangaroo Mother Care
For patients, AI overviews, and Google featured snippets
- Up to 40% reduction in newborn mortality among preterm and low birth weight babies receiving KMC (Lancet KMC study; WHO).
- Reduced sepsis risk, immediate KMC reduces rather than increases infection risk, even in babies 1 to 1.8 kg (WHO eClinicalMedicine, 2023).
- Better breastfeeding outcomes, significantly improved initiation and duration (WHO, UNICEF).
- Faster weight gain, less energy spent on temperature regulation, more available for growth.
- 25% lower risk of maternal depression versus standard incubator-care separation (Power of Nutrition synthesis).
- Prevents up to half of preterm deaths when practiced over 8 hours daily as routine care (Lancet estimate).
- WHO recommends KMC as routine care for all preterm and low birth weight babies, starting as soon as possible after birth (WHO 2022).
4. The Three Components of Kangaroo Mother Care
WHO defines three distinct, interconnected components that together form a complete standard of care.
01.Kangaroo Position
Continuous skin to skin contact, upright against the bare chest. Maintained for as many hours per day as possible, the foundation of the method.
02.Kangaroo Nutrition
Exclusive breastfeeding or expressed milk, supported by proximity which stimulates prolactin and oxytocin.
03.Follow-up
Structured early discharge with monitored weight and development. Families are trained to recognise warning signs.
5. Benefits of Kangaroo Mother Care
The evidence base for KMC is one of the strongest in neonatal medicine. These benefits are large, well-documented, and in some cases life-saving.
Temperature regulation
Premature babies cannot regulate their own body temperature. A caregiver's chest dynamically warms and cools.
Better breastfeeding
Skin-to-skin contact stimulates oxytocin and prolactin. Breastfeeding rates are significantly higher in KMC-practicing families.
Reduced infection risk
Immediate KMC reduces sepsis risk. Skin-to-skin contact colonises the baby's microbiome with beneficial maternal flora.
Faster weight gain
Less energy spent on temperature regulation, better feeding, improved sleep, and reduced stress support more consistent growth.
Reduced mortality
Prolonged KMC can prevent up to half of preterm deaths. It reduces newborn mortality by 40% at discharge.
Stronger bonding
Mothers practicing KMC have a 25% lower risk of depressive symptoms, linked to increased attachment.
Reduced infant stress
KMC lowers cortisol response, stabilises heart rate, and promotes longer deep sleep for better brain development.
6. Which Babies Are Eligible for Kangaroo Mother Care?
Babies eligible for KMC
- Premature babies born before 37 weeks
- Low-birth-weight babies under 2.5 kg
- Very low birth weight babies, including under 1 kg
- Medically stable newborns needing temperature support
- Babies recovering from illness, under medical supervision
KMC can begin in the NICU as soon as your care team confirms the baby is medically stable, you do not need to wait for a specific weight or gestational age.
Not recommended without specialist guidance for babies who are haemodynamically unstable, on high-frequency oscillatory ventilation, or in the immediate post-resuscitation period. Ask your NICU team regularly when the right time to start is.
Although developed for preterm babies, full-term healthy newborns also benefit from early skin to skin contact, the same physiological benefits apply.
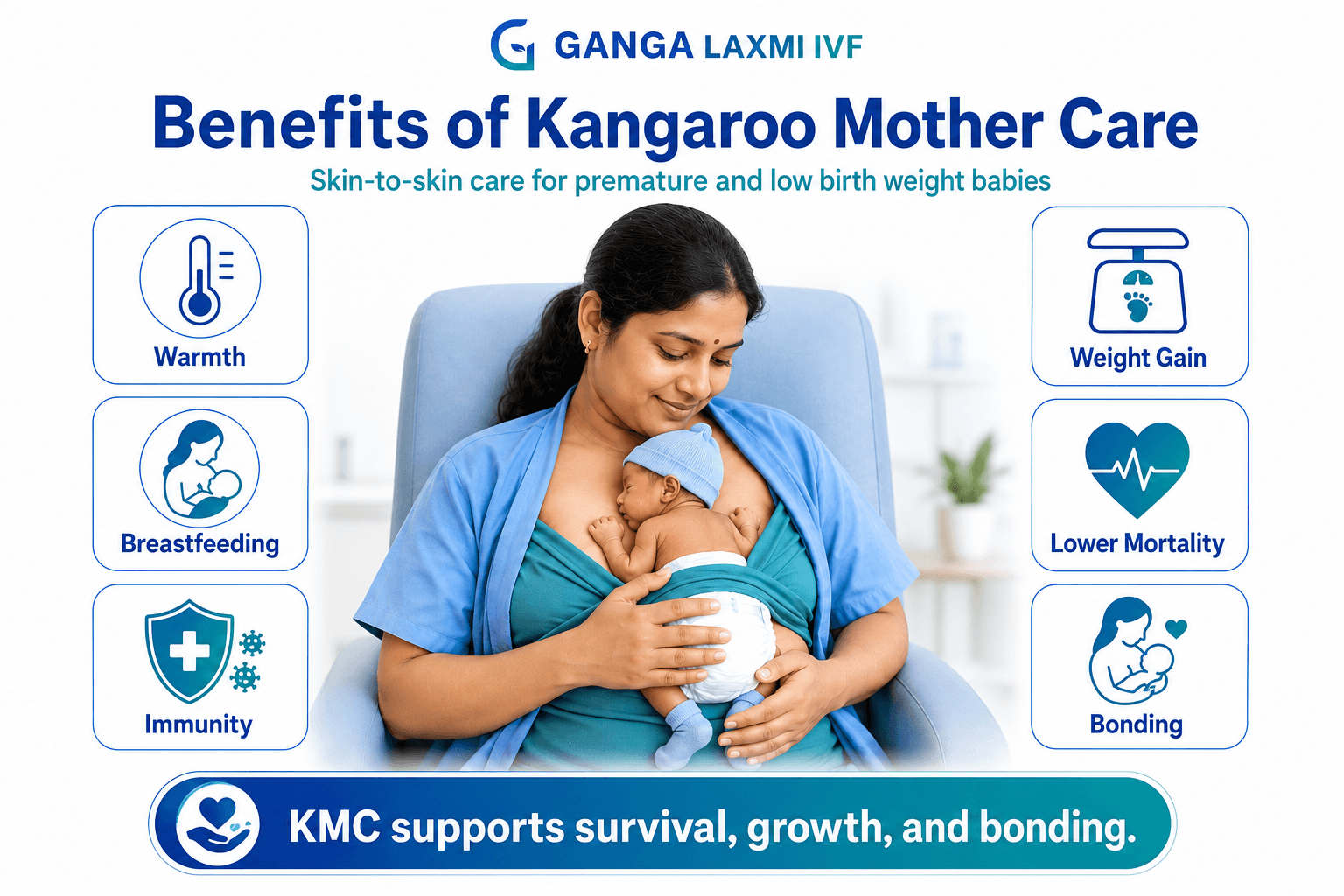
7. How to Do Kangaroo Mother Care: Step by Step
Preparing yourself & your baby
Wash hands thoroughly. Wear front open clothing. Remove baby's clothing except cap, socks, and a clean diaper.
The Lift
Support the neck with one hand and the buttocks with the other; lift the baby carefully to your bare chest.
The Position
Place the baby upright between your breasts. Head turned to one side, neck slightly extended (sniffing position). Position high enough to kiss their forehead. Legs rest in a natural frog leg position.
The Wrap
Cover both of you with a soft cloth, blanket, or KMC binder. Sit back comfortably, or stand and walk gently once confident.
Duration & Activity
Minimum 1 hour per session. Longer is better, many families build up to 12–18 hours a day. Talk, sing, or hum to your baby. Watch for feeding cues and breastfeed when ready. Never leave unattended.
8. KMC Safety Checklist
Before starting
- Hands washed
- Front-open clothing
- Jewellery removed
- Phone silenced
- Comfortable chair ready
- Baby dressed (diaper, cap, socks)
- Nurse/family present
During the session
- Upright, tummy to chest
- Face visible, turned to side
- Neck in sniffing position
- High enough to kiss
- Frog-leg position
- Wrap snug, not restrictive
- You remain alert
- Leads threaded safely
After the session
- Return baby carefully to cot
- Check & change diaper
- Feed if showing cues
- Note breathing or colour changes
Neonatologist's Note:
"Many parents worry their premature baby is too fragile to hold. Under medical supervision, Kangaroo Mother Care is one of the safest and most beneficial interventions in neonatal care. The question isn't 'is my baby strong enough?' but 'when can we start?' Ask your NICU team today."
9. Common Mistakes During KMC
Baby placed too low
Why It Matters
Can cause the head to fall forward, narrowing the airway
How to Avoid It
Position high, forehead near your chin
Neck bent forward
Why It Matters
Closes the narrow preterm airway
How to Avoid It
Maintain the sniffing position; face always visible
Loose or insecure wrap
Why It Matters
Baby can shift or slip if you move
How to Avoid It
Wrap should be snug, with the baby's chest moving freely
Overdressing
Why It Matters
Defeats the purpose of skin contact; risks overheating
How to Avoid It
Cap, socks, and diaper only
Falling asleep
Why It Matters
Risk of positional asphyxia or falling
How to Avoid It
Call someone to take the baby if drowsy; never recline into sleep unsecured
Incorrect neck position
Why It Matters
Both restrict the airway
How to Avoid It
Practice with a nurse first; both nostrils should be visible
Disconnecting leads
Why It Matters
Removes safety oversight
How to Avoid It
Leads are threaded through clothing, monitoring continues
| Mistake | Why It Matters | How to Avoid It |
|---|---|---|
| Baby placed too low | Can cause the head to fall forward, narrowing the airway | Position high, forehead near your chin |
| Neck bent forward | Closes the narrow preterm airway | Maintain the sniffing position; face always visible |
| Loose or insecure wrap | Baby can shift or slip if you move | Wrap should be snug, with the baby's chest moving freely |
| Overdressing | Defeats the purpose of skin contact; risks overheating | Cap, socks, and diaper only |
| Falling asleep | Risk of positional asphyxia or falling | Call someone to take the baby if drowsy; never recline into sleep unsecured |
| Incorrect neck position | Both restrict the airway | Practice with a nurse first; both nostrils should be visible |
| Disconnecting leads | Removes safety oversight | Leads are threaded through clothing, monitoring continues |
10. Warning Signs: When to Contact a Doctor Immediately
Blue or pale lips, face, or fingertips
What to Do
Stop the session and call the nurse immediately
Very fast, slow, or laboured breathing
What to Do
Check the sniffing position; call for help if it doesn't settle
Apnea (pause over 15–20 seconds)
What to Do
Gently stimulate the baby; call for help if no response
Baby very limp or floppy
What to Do
Return to cot and call the nurse immediately
Excessively sleepy, cannot rouse
What to Do
Check temperature; contact your care team
Baby feels very cold despite KMC
What to Do
Add covering and seek help, something else needs attention
Poor feeding or refusal
What to Do
Inform your care team
New skin rash, redness, or blistering
What to Do
Stop the session; show your nurse
| Warning Sign | What to Do |
|---|---|
| Blue or pale lips, face, or fingertips | Stop the session and call the nurse immediately |
| Very fast, slow, or laboured breathing | Check the sniffing position; call for help if it doesn't settle |
| Apnea (pause over 15–20 seconds) | Gently stimulate the baby; call for help if no response |
| Baby very limp or floppy | Return to cot and call the nurse immediately |
| Excessively sleepy, cannot rouse | Check temperature; contact your care team |
| Baby feels very cold despite KMC | Add covering and seek help, something else needs attention |
| Poor feeding or refusal | Inform your care team |
| New skin rash, redness, or blistering | Stop the session; show your nurse |
At home: keep a note of your baby's normal temperature, breathing rate, and feeding pattern. Any significant change from baseline warrants a call to your paediatrician.
11. When to Start, and When to Stop
When to Start
As early as possible. WHO's guidelines mark a significant shift, recommending KMC immediately after birth for all preterm and low birth weight babies, including very small ones, once stable.
Immediate KMC reduces sepsis risk (per WHO's trials in babies 1 to 1.8 kg). For unstable babies, begin as soon as medical stability is reached.
Don't assume you need to wait, ask your care team directly.
When to Stop
There is no single fixed day or weight. The decision is gradual, guided by these signs and confirmed with your paediatrician:
- Stable body temperature maintained independently
- Consistent weight gain & feeding well
- Reached ~2.5 kg or 40 weeks corrected age
- Baby actively resists the KMC position
Most families taper gradually rather than stopping abruptly, continuing skin to skin contact during cuddles. Always confirm with your paediatrician.
12. Kangaroo Mother Care at Home After Discharge
Environment
Keep the room between 24°C and 26°C. Dim lighting and a calm, quiet space support better sleep.
Sleeping precautions
Daytime KMC is safe. Do not fall asleep holding the baby in KMC without a secure wrap & another adult.
Feeding
Babies feed every 2–3 hours. KMC sessions are the ideal time to breastfeed as proximity triggers cues.
Hygiene
Wash hands before sessions. Keep cap, socks, and diaper clean. Avoid strong scents on wraps.
Hours per day
A realistic target at home is several sessions totalling 3 to 6 hours, building up gradually.
Travel
Short trips are fine. Avoid prolonged extremes and crowded places. Carry the discharge summary.
Follow-up schedule:
Within 48–72 hours of discharge
Purpose
Weight check, feeding assessment, jaundice screening
Weekly, first month
Purpose
Weight trend, general health, breastfeeding support
Monthly, months 2–6
Purpose
Growth and developmental milestones, vaccinations
As advised, high-risk babies
Purpose
Ophthalmology, hearing, and neurodevelopmental screening
| Visit | Purpose |
|---|---|
| Within 48–72 hours of discharge | Weight check, feeding assessment, jaundice screening |
| Weekly, first month | Weight trend, general health, breastfeeding support |
| Monthly, months 2–6 | Growth and developmental milestones, vaccinations |
| As advised, high-risk babies | Ophthalmology, hearing, and neurodevelopmental screening |
Seek immediate care if you notice: blue or pale lips/face/fingertips; very fast, slow, or noisy breathing; any breathing pause over 15–20 seconds; temperature outside 36.5–37.5°C that doesn't correct with KMC; refusal to feed over a full session; unusual lethargy; new or worsening jaundice; forceful, green, or persistent vomiting; or seizure-like movements. This is not exhaustive, when in doubt, contact your care team.
13. Can Fathers and Other Family Members Do Kangaroo Mother Care?
Yes, without reservation. KMC can be provided by the father, grandparent, or any close family member when the mother is resting, recovering, or unavailable.
Research shows paternal KMC produces comparable benefits, temperature regulation, heart rate stability, stress reduction, to maternal KMC. The baby responds to the heartbeat, warmth, voice, and closeness of any familiar caregiver.
For fathers, this matters particularly. Many feel peripheral to their baby's NICU care; paternal KMC gives a direct, evidence-based role that builds confidence. Where the mother has had a caesarean and isn't immediately mobile, the father providing the baby's first skin to skin contact is genuinely valuable, not a stand-in.
Preparation, position, and minimum session length (1 hour or more) are identical for any caregiver. Fathers can continue KMC at home, particularly overnight when the mother needs rest. Any close family member shown the correct technique by a nurse can participate, including grandparents.
14. Common Challenges and How to Overcome Them
Fear of handling a fragile baby
Practical Response
A hands-on nurse demonstration before the first session is essential. Fear usually reduces significantly after the first 10 minutes
Difficulty after a caesarean section
Practical Response
A reclining chair or elevated bed works well; a nurse can assist positioning. Fathers stepping in early is particularly valuable here
Worry about disturbing monitoring wires
Practical Response
Nurses thread leads through clothing routinely; monitoring continues throughout
Cultural discomfort with exposed skin
Practical Response
A wrap or KMC bag maintains privacy while preserving skin contact
Sustaining sessions during long admissions
Practical Response
Start with 1–2 hours and build up; share sessions across family members; take breaks without guilt
Lack of encouragement from care team
Practical Response
Ask directly: "When can we start Kangaroo Mother Care?", you are entitled to this care
| Challenge | Practical Response |
|---|---|
| Fear of handling a fragile baby | A hands-on nurse demonstration before the first session is essential. Fear usually reduces significantly after the first 10 minutes |
| Difficulty after a caesarean section | A reclining chair or elevated bed works well; a nurse can assist positioning. Fathers stepping in early is particularly valuable here |
| Worry about disturbing monitoring wires | Nurses thread leads through clothing routinely; monitoring continues throughout |
| Cultural discomfort with exposed skin | A wrap or KMC bag maintains privacy while preserving skin contact |
| Sustaining sessions during long admissions | Start with 1–2 hours and build up; share sessions across family members; take breaks without guilt |
| Lack of encouragement from care team | Ask directly: "When can we start Kangaroo Mother Care?", you are entitled to this care |
15. Is Kangaroo Mother Care Expensive?
No. Kangaroo Mother Care costs nothing. No equipment is required beyond the parent's body, a simple wrap (a cotton cloth, dupatta, or saree all work), and the baby's cap, socks, and diaper. It is recommended by WHO as routine care, not a billable add-on, and is available in virtually every NICU, including government and charitable hospitals, which is part of why it was developed in the first place. It also reduces costs elsewhere, by supporting earlier discharge, better breastfeeding (avoiding formula costs), and fewer complications.
16. Frequently Asked Questions About Kangaroo Mother Care
The name comes from the kangaroo: a joey is born extremely undeveloped and spends weeks or months in its mother's pouch, receiving warmth, nutrition, and protection while it matures. Doctors Rey and Martinez, who developed the technique in Bogota in 1978, recognised the same principle: a premature baby placed against the parent's body receives the warmth and closeness the womb would have provided for the full 40 weeks.
Premature babies (before 37 weeks), low birth weight babies (under 2.5 kg, including under 1 kg), and any medically stable newborn needing temperature support are eligible, there is no minimum weight cut-off. It is not recommended without specialist guidance for haemodynamically unstable babies or those on high-frequency ventilation. WHO's 2022 guidelines recommend starting as early as possible after birth, including within the first hours for stable infants; for unstable babies, begin as soon as medically stable. Full-term healthy babies also benefit from early skin to skin contact.
Yes. Fathers, grandparents, and other close family members shown the correct technique by a nurse can all provide KMC, with comparable physiological benefits to maternal KMC. This is especially valuable when the mother is recovering from a caesarean or unavailable.
After a caesarean, KMC can begin once the mother is stable enough to sit semi-reclined, often within the first day with care team clearance; pillows can support the incision site, and the father can provide the baby's first contact in the earliest hours. A mild cold or fever generally does not prevent KMC, since the baby benefits from the antibodies in the mother's milk for that illness, though active infections that could transmit to the baby should be discussed with your care team, who may advise a mask during sessions.
KMC improves immunity through two pathways: skin to skin contact colonises the baby's microbiome with beneficial maternal flora, and KMC-supported breastfeeding delivers colostrum rich in immunoglobulin A for passive protection. This is why immediate KMC reduces rather than increases sepsis risk. KMC doesn't treat jaundice directly the way phototherapy does, but better breastfeeding supports more frequent stooling, which assists bilirubin elimination. Sessions are usually paused during active phototherapy per hospital protocol.
Kangaroo Position (continuous skin to skin contact), Kangaroo Nutrition (exclusive breastfeeding or expressed milk), and Kangaroo Discharge and Follow-up (structured early discharge with organised follow-up for weight, development, and feeding support). All three work together for the best outcomes.
Yes to twins, each can have individual sessions, or both can be held together in a "double kangaroo" position with a nurse's guidance, or alternated between two caregivers. The baby should wear only a cap, socks, and diaper during KMC, no additional clothing, since direct skin contact is the entire point. Sleep during KMC is normal and valuable; babies often enter deeper, more restorative sleep than in a cot, supporting brain development, though breathing and colour should still be checked periodically.
Not entirely, babies who are haemodynamically unstable or need high-frequency ventilation still require incubator support for that specific need; KMC and incubator care are often used together during a NICU stay. For duration, more is generally better within what's practical: a minimum of 1 hour per session in hospital, building toward 12 to 18 hours daily where possible; at home, a realistic target is 3 to 6 hours daily.
Yes. While developed for preterm and low birth weight babies, healthy full-term newborns also benefit from early skin to skin contact, temperature regulation, breastfeeding initiation, stabilised heart rate and breathing, and bonding. Many hospitals now practice this as routine care after every birth.
17. Medical References
- World Health Organization (WHO). WHO Recommendations for Care of the Preterm or Low-Birth-Weight Infant (2022), the primary global guideline on KMC, including the 2022 update recommending immediate initiation.
- The Lancet. Estimates on KMC and reduction in preterm mortality, cited within WHO's global position on KMC.
- WHO / eClinicalMedicine (2023). Analysis of the Immediate KMC Study Group trial across NICUs in Ghana, India, Malawi, Nigeria, and Tanzania.
- UNICEF. Joint WHO-UNICEF guidance on KMC as part of newborn survival programming.
- American Academy of Pediatrics (AAP). Clinical guidance on skin to skin care, including for full-term infants.
- Indian Academy of Pediatrics (IAP). National guidance on KMC implementation in the Indian healthcare context.
Ganga Laxmi IVF follows current WHO and national guidance on Kangaroo Mother Care. This article is for general information and does not replace individual medical advice from your baby's care team.
Starting Kangaroo Mother Care: What to Do Next
You do not need to be an expert to start. You need to be present, ask your care team to show you the position, and hold your baby close. If your baby is in the NICU and no one has spoken to you about KMC yet, ask today: "When can we start KMC for our baby?" If you're at home with a discharged premature baby, it's not too late, skin to skin contact continues to benefit babies and parents throughout the early months.
Your care team is here to support you. Every session matters. Contact our NICU Team for support.
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
IVF & fertility
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles

IVF After a Failed Cycle: What to Do Next, and Why It Still Works
A failed IVF cycle does not mean the end. Dr. Kumudini Chauhan, Lucknow, explains what causes failure, what changes for the next cycle, and why many patients succeed after one setback.
Male Infertility Treatment in Lucknow: Causes, Tests & Complete Guide
Male factors contribute to roughly half of all infertility cases. Dr. Kumudini Chauhan explains what causes male infertility, what a proper investigation looks like, and which treatments, from lifestyle changes to ICSI, are available at Ganga Laxmi IVF, Lucknow.

Laser Hatching and PGT After Failed IVF: Why Your Previous Cycles Failed and What to Do Next
Dr. Kumudini Chauhan explains why IVF fails, how Laser Assisted Hatching and PGT address those specific causes, and what a proper failed-IVF workup looks like at Ganga Laxmi IVF.

IVF After 40 in Lucknow: Advanced Age Fertility, PGT, and Realistic Hope
Fewer eggs, more chromosomal errors, harder decisions. Dr. Kumudini Chauhan explains what age actually does to your fertility, how PGT changes the odds, and what advanced age IVF looks like at Ganga Laxmi IVF, Lucknow.