In my twenty years of practice in Lucknow, one of the most persistent and damaging misconceptions I encounter is this: that infertility is a woman's problem. It is not. Roughly 40 to 50 percent of all infertility cases involve a male factor, either alone or in combination with a female factor. Yet men are far less likely to seek evaluation, and far more likely to carry the weight of the diagnosis silently.
I want to say this directly and without any ambiguity: male infertility is a medical condition. It has medical solutions. And the most powerful of those solutions is ICSI.
Intracytoplasmic Sperm Injection, or ICSI, has fundamentally changed what is possible in fertility medicine. Men who were once told they could never father children now do so routinely. Men with extremely low sperm counts, very poor motility, abnormal morphology, or even no sperm in their ejaculate at all have become fathers through ICSI. This article explains how it works, who needs it, and what you can expect at Ganga Laxmi IVF.
Key fact
ICSI requires only a single viable sperm to fertilise each egg.
The total number of sperm in a semen sample, which can feel like a devastating number when low, becomes almost irrelevant when a skilled embryologist can select one healthy sperm and inject it directly into one mature egg.
What Is ICSI and How Is It Different from Standard IVF?
Both ICSI and standard IVF are forms of assisted reproduction where fertilisation takes place in an embryology laboratory rather than inside the body. The critical difference lies in how fertilisation is achieved.
In standard IVF, retrieved eggs and a prepared sperm sample are placed together in a culture dish and incubated. Fertilisation occurs when a sperm successfully penetrates the egg on its own. This requires thousands of motile sperm competing to reach and fertilise each egg.
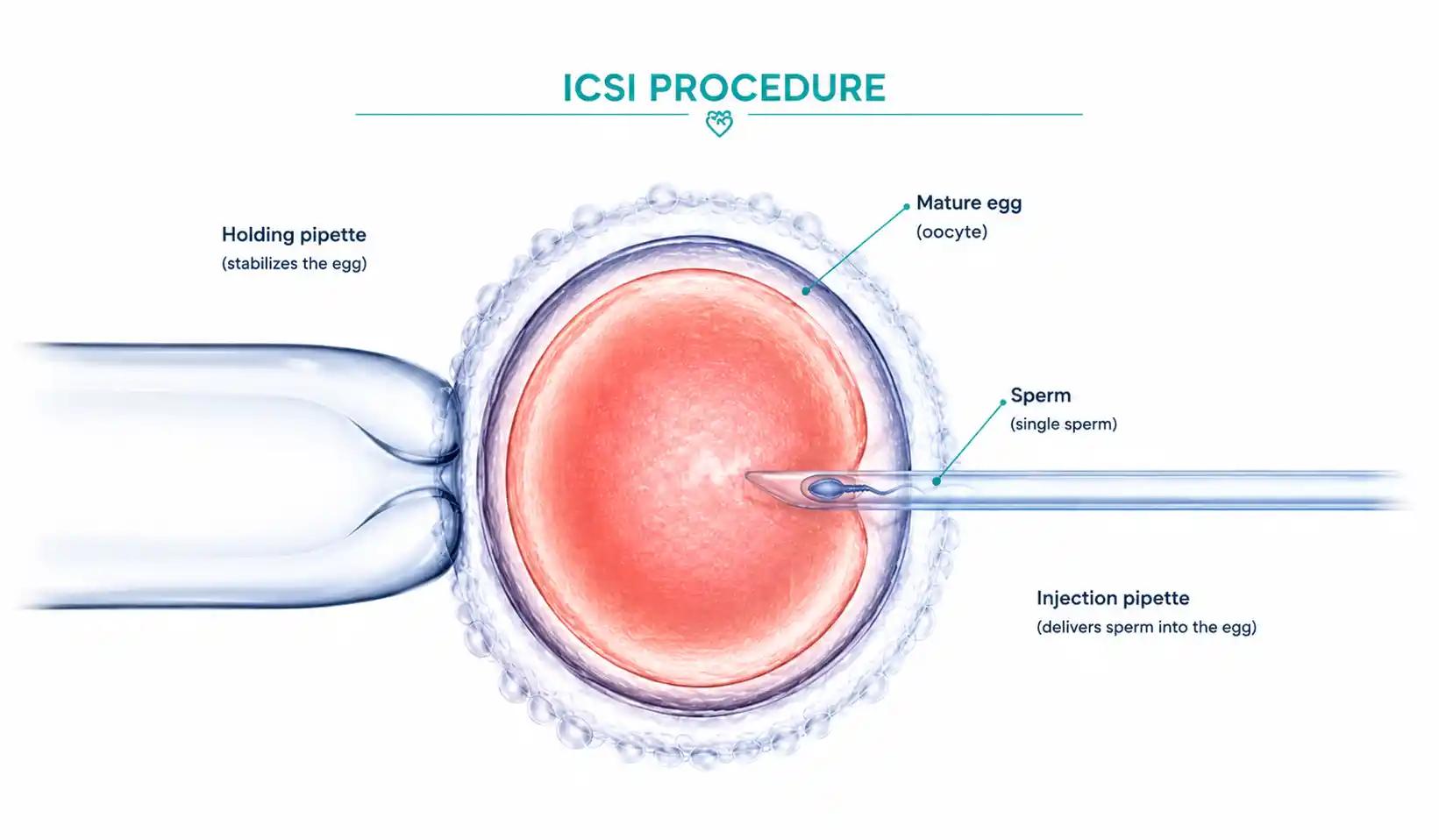
In ICSI, a single sperm is selected under high-powered magnification, immobilised carefully, and injected directly through the outer coat of the egg into the cytoplasm using an ultra-fine glass needle. Fertilisation does not depend on the sperm's ability to swim, penetrate, or compete. The embryologist does what the sperm cannot.
The fertilised egg is then cultured in the laboratory for three to five days and the healthiest resulting embryo is transferred into the uterus. From that point forward, the process is identical to a standard IVF cycle.
IVF vs ICSI: Side-by-Side Comparison
Process
Standard IVF
Sperm and eggs placed together in a dish; fertilisation happens naturally in the lab.
ICSI
A single sperm is selected and injected directly into each mature egg using a microscopic needle.
Sperm Requirement
Standard IVF
Thousands of motile sperm needed for each egg.
ICSI
A single viable sperm is sufficient for each egg.
Best For
Standard IVF
Mild male factor or no male factor; good sperm parameters.
ICSI
Low sperm count, low motility, abnormal morphology, azoospermia, or failed IVF fertilisation.
Fertilisation Rate
Standard IVF
Variable; depends on sperm quality.
ICSI
Typically 70 to 85% of mature eggs fertilise successfully.
Embryo Transfer
Standard IVF
Same as ICSI: embryo placed directly into the uterus.
ICSI
Same as standard IVF: embryo placed directly into the uterus.
When Dr. Chauhan Recommends It
Standard IVF
When sperm parameters are within normal range.
ICSI
When male factor is present, or as a precaution in selected cases to maximise fertilisation.
| Factor | Standard IVF | ICSI |
|---|---|---|
| Process | Sperm and eggs placed together in a dish; fertilisation happens naturally in the lab. | A single sperm is selected and injected directly into each mature egg using a microscopic needle. |
| Sperm Requirement | Thousands of motile sperm needed for each egg. | A single viable sperm is sufficient for each egg. |
| Best For | Mild male factor or no male factor; good sperm parameters. | Low sperm count, low motility, abnormal morphology, azoospermia, or failed IVF fertilisation. |
| Fertilisation Rate | Variable; depends on sperm quality. | Typically 70 to 85% of mature eggs fertilise successfully. |
| Embryo Transfer | Same as ICSI: embryo placed directly into the uterus. | Same as standard IVF: embryo placed directly into the uterus. |
| When Dr. Chauhan Recommends It | When sperm parameters are within normal range. | When male factor is present, or as a precaution in selected cases to maximise fertilisation. |
Important clinical note
ICSI is not automatically better than standard IVF for every patient. When sperm parameters are normal, standard IVF is entirely appropriate and equally effective. Dr. Chauhan recommends ICSI only when there is a clinical reason to do so, protecting patients from unnecessary procedures and cost.
Who Needs ICSI? Conditions and Indications
ICSI is recommended when the sperm's ability to fertilise an egg independently is compromised in any way, or when previous attempts at fertilisation have failed. The table below outlines the main indications using current WHO 2021 semen analysis reference values.
Low Sperm Count
Medical Term
Oligospermia
What It Means
Fewer than 15 million sperm per mL of semen (WHO 2021 reference value).
ICSI Outcome
Single viable sperm selected per egg; count is no longer the limiting factor.
Low Sperm Motility
Medical Term
Asthenospermia
What It Means
Less than 30% of sperm showing progressive motility (WHO 2021 reference value).
ICSI Outcome
The embryologist selects the most motile sperm available under high magnification.
Abnormal Sperm Shape
Medical Term
Teratospermia
What It Means
Less than 4% normal morphology (Kruger strict criteria).
ICSI Outcome
Morphology matters less when a single normal-looking sperm is hand-selected.
No Sperm in Ejaculate
Medical Term
Azoospermia
What It Means
Complete absence of sperm in the ejaculate.
ICSI Outcome
Sperm retrieved surgically via TESA or PESA and used directly in ICSI.
Failed IVF Fertilisation
Medical Term
Fertilisation failure
What It Means
Previous IVF cycle produced eggs but no fertilisation.
ICSI Outcome
ICSI bypasses the barrier that prevented fertilisation in standard IVF.
Unexplained Infertility
Medical Term
Idiopathic
What It Means
All standard tests normal but pregnancy not occurring.
ICSI Outcome
ICSI used after failed IUI cycles and where IVF alone has not resulted in fertilisation.
Very Low Egg Yield
Medical Term
Poor responder
What It Means
Few mature eggs retrieved in stimulation cycle.
ICSI Outcome
ICSI maximises fertilisation from every available egg, which is critical when eggs are scarce.
| Condition | Medical Term | What It Means | ICSI Outcome |
|---|---|---|---|
| Low Sperm Count | Oligospermia | Fewer than 15 million sperm per mL of semen (WHO 2021 reference value). | Single viable sperm selected per egg; count is no longer the limiting factor. |
| Low Sperm Motility | Asthenospermia | Less than 30% of sperm showing progressive motility (WHO 2021 reference value). | The embryologist selects the most motile sperm available under high magnification. |
| Abnormal Sperm Shape | Teratospermia | Less than 4% normal morphology (Kruger strict criteria). | Morphology matters less when a single normal-looking sperm is hand-selected. |
| No Sperm in Ejaculate | Azoospermia | Complete absence of sperm in the ejaculate. | Sperm retrieved surgically via TESA or PESA and used directly in ICSI. |
| Failed IVF Fertilisation | Fertilisation failure | Previous IVF cycle produced eggs but no fertilisation. | ICSI bypasses the barrier that prevented fertilisation in standard IVF. |
| Unexplained Infertility | Idiopathic | All standard tests normal but pregnancy not occurring. | ICSI used after failed IUI cycles and where IVF alone has not resulted in fertilisation. |
| Very Low Egg Yield | Poor responder | Few mature eggs retrieved in stimulation cycle. | ICSI maximises fertilisation from every available egg, which is critical when eggs are scarce. |
It is important to note that a single abnormal semen analysis result does not define a man's fertility permanently. Sperm parameters can fluctuate based on illness, stress, heat exposure, and other factors. Dr. Chauhan always reviews at least two semen analyses before making a treatment recommendation, and interprets results in full clinical context rather than in isolation.
ICSI for Low Sperm Count and Low Sperm Motility
Low sperm count and low sperm motility are the two most common male factor diagnoses I see in my practice in Lucknow. Both were, until relatively recently, associated with very limited treatment options. ICSI changed that completely.
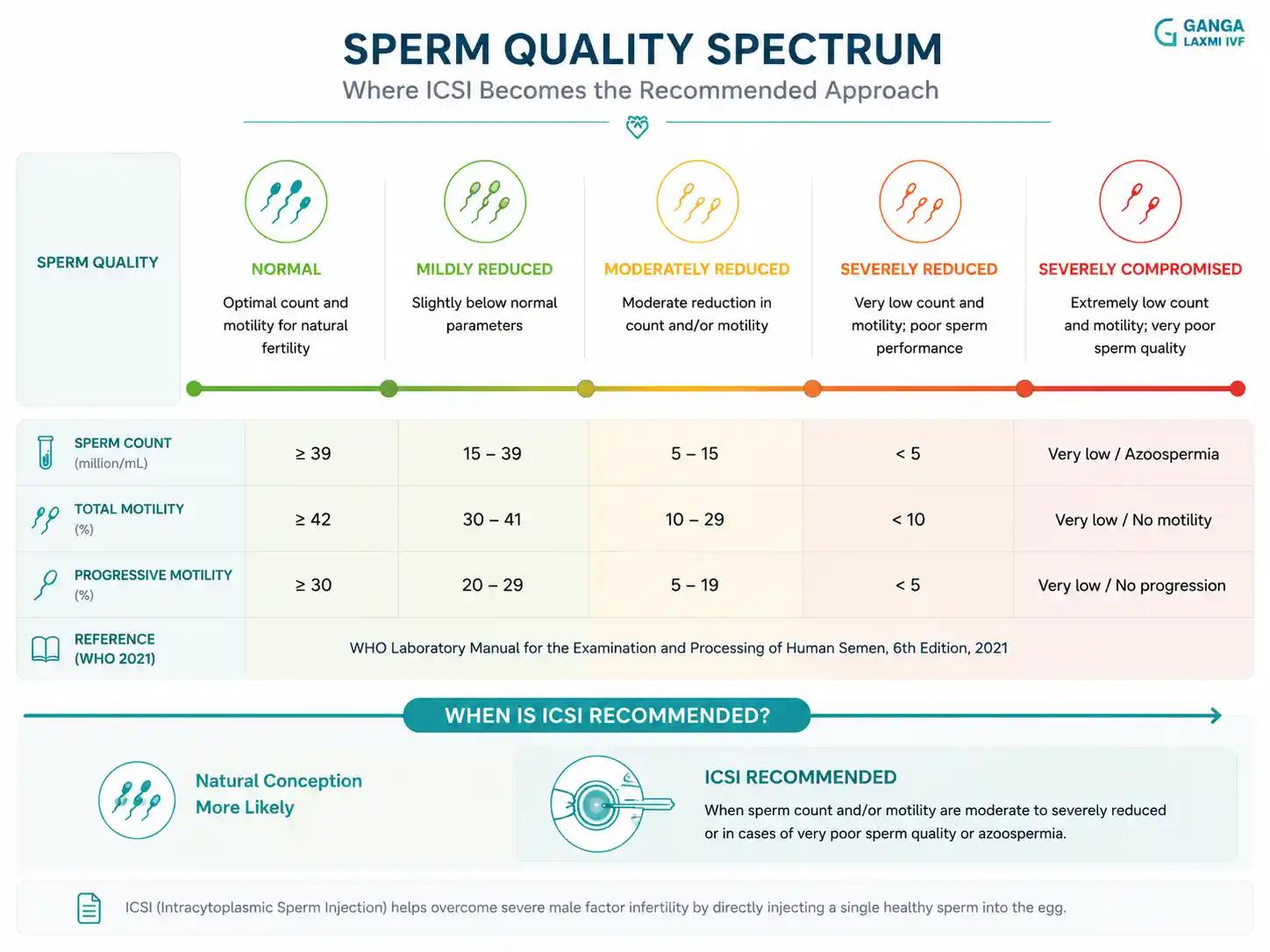
WHO 2021 Sperm Parameter Reference Values and Clinical Implications
Sperm Concentration
WHO 2021 Lower Reference Limit
16 million per mL
Clinical Implication if Below Threshold
Oligospermia. IVF fertilisation rates decline sharply. ICSI strongly recommended.
Total Motility
WHO 2021 Lower Reference Limit
42% (progressive + non-progressive)
Clinical Implication if Below Threshold
Asthenospermia. Reduces sperm-egg contact in standard IVF. ICSI selects best available.
Progressive Motility
WHO 2021 Lower Reference Limit
30%
Clinical Implication if Below Threshold
Sperm not swimming forward efficiently. ICSI bypasses the need for sperm to self-navigate.
Normal Morphology
WHO 2021 Lower Reference Limit
4% (Kruger strict criteria)
Clinical Implication if Below Threshold
Teratospermia. Shape affects ability to penetrate the egg. ICSI injects sperm directly.
Total Sperm Count
WHO 2021 Lower Reference Limit
39 million per ejaculate
Clinical Implication if Below Threshold
Below this, ICSI is the preferred fertilisation method regardless of other parameters.
| Parameter | WHO 2021 Lower Reference Limit | Clinical Implication if Below Threshold |
|---|---|---|
| Sperm Concentration | 16 million per mL | Oligospermia. IVF fertilisation rates decline sharply. ICSI strongly recommended. |
| Total Motility | 42% (progressive + non-progressive) | Asthenospermia. Reduces sperm-egg contact in standard IVF. ICSI selects best available. |
| Progressive Motility | 30% | Sperm not swimming forward efficiently. ICSI bypasses the need for sperm to self-navigate. |
| Normal Morphology | 4% (Kruger strict criteria) | Teratospermia. Shape affects ability to penetrate the egg. ICSI injects sperm directly. |
| Total Sperm Count | 39 million per ejaculate | Below this, ICSI is the preferred fertilisation method regardless of other parameters. |
In standard IVF or natural conception, sperm with low count and poor motility simply cannot reach the egg in sufficient numbers or swim effectively enough to penetrate it. ICSI removes both barriers entirely. The embryologist examines the sample under high magnification, identifies the sperm with the best morphology and any visible forward movement, and selects that single cell for injection.
Even in samples with counts as low as a few hundred thousand per mL, or with predominantly immotile sperm, it is often possible to identify viable cells suitable for ICSI. I have seen patients with severely compromised semen analyses achieve fertilisation, healthy embryos, and successful pregnancies through ICSI at Ganga Laxmi IVF. This is not exceptional. It is what ICSI was designed to accomplish.
A Note on DNA Fragmentation
In some cases of poor sperm parameters, particularly when ICSI cycles have resulted in poor embryo quality or recurrent implantation failure, Dr. Chauhan may recommend a sperm DNA fragmentation test. High DNA fragmentation can affect embryo development even when fertilisation occurs normally.
If DNA fragmentation is elevated, options including testicular sperm extraction (TESA), antioxidant therapy, or modified ICSI protocols may be discussed. This is an individualised decision based on your complete clinical picture.
ICSI in Unexplained Infertility
Unexplained infertility is one of the most frustrating diagnoses a couple can receive. All standard investigations come back within normal range: the tubes are open, ovulation is confirmed, semen analysis appears adequate, and yet pregnancy does not happen.
In a significant proportion of these cases, the barrier is at the level of fertilisation itself. Something prevents the sperm from successfully penetrating the egg, even though neither the sperm nor the egg appears abnormal on standard testing. This is called unexplained fertilisation failure, and it is only identifiable once an IVF cycle is attempted and fertilisation does not occur.
The Treatment Pathway for Unexplained Infertility
At Ganga Laxmi IVF, unexplained infertility is managed in a stepwise way, moving from the least invasive option to more targeted treatment based on response.
Step Step 1 — IUI
Method
IUI
Full Name
Intrauterine Insemination
When It Is Used
Least invasive. Washed sperm placed directly in uterus. Recommended first when tubes are open and sperm parameters are acceptable.
Step Step 2 — IVF
Method
IVF
Full Name
In Vitro Fertilisation
When It Is Used
Eggs retrieved and fertilised in lab with standard insemination. Appropriate when IUI has failed or female factors are present.
Step Step 3 — ICSI
Method
ICSI
Full Name
Intracytoplasmic Sperm Injection
When It Is Used
Single sperm injected into each egg. Recommended when male factor is confirmed, IVF fertilisation has failed, or unexplained infertility persists after IVF.
| Step | Method | Full Name | When It Is Used |
|---|---|---|---|
| Step 1 | IUI | Intrauterine Insemination | Least invasive. Washed sperm placed directly in uterus. Recommended first when tubes are open and sperm parameters are acceptable. |
| Step 2 | IVF | In Vitro Fertilisation | Eggs retrieved and fertilised in lab with standard insemination. Appropriate when IUI has failed or female factors are present. |
| Step 3 | ICSI | Intracytoplasmic Sperm Injection | Single sperm injected into each egg. Recommended when male factor is confirmed, IVF fertilisation has failed, or unexplained infertility persists after IVF. |
When a couple reaches Step 3, ICSI resolves unexplained fertilisation failure in a large majority of cases. By physically placing the sperm inside the egg, it bypasses whatever subtle biological barrier was preventing fertilisation. The resulting embryos are then transferred in exactly the same way as in any other IVF cycle.
If you have experienced repeated IUI failures and have been advised to consider IVF, it is worth having a frank discussion with Dr. Chauhan about whether ICSI rather than standard IVF is the more appropriate first choice for your situation. You may also find our guide on IVF for tubal block helpful if tubal factors are part of your picture.
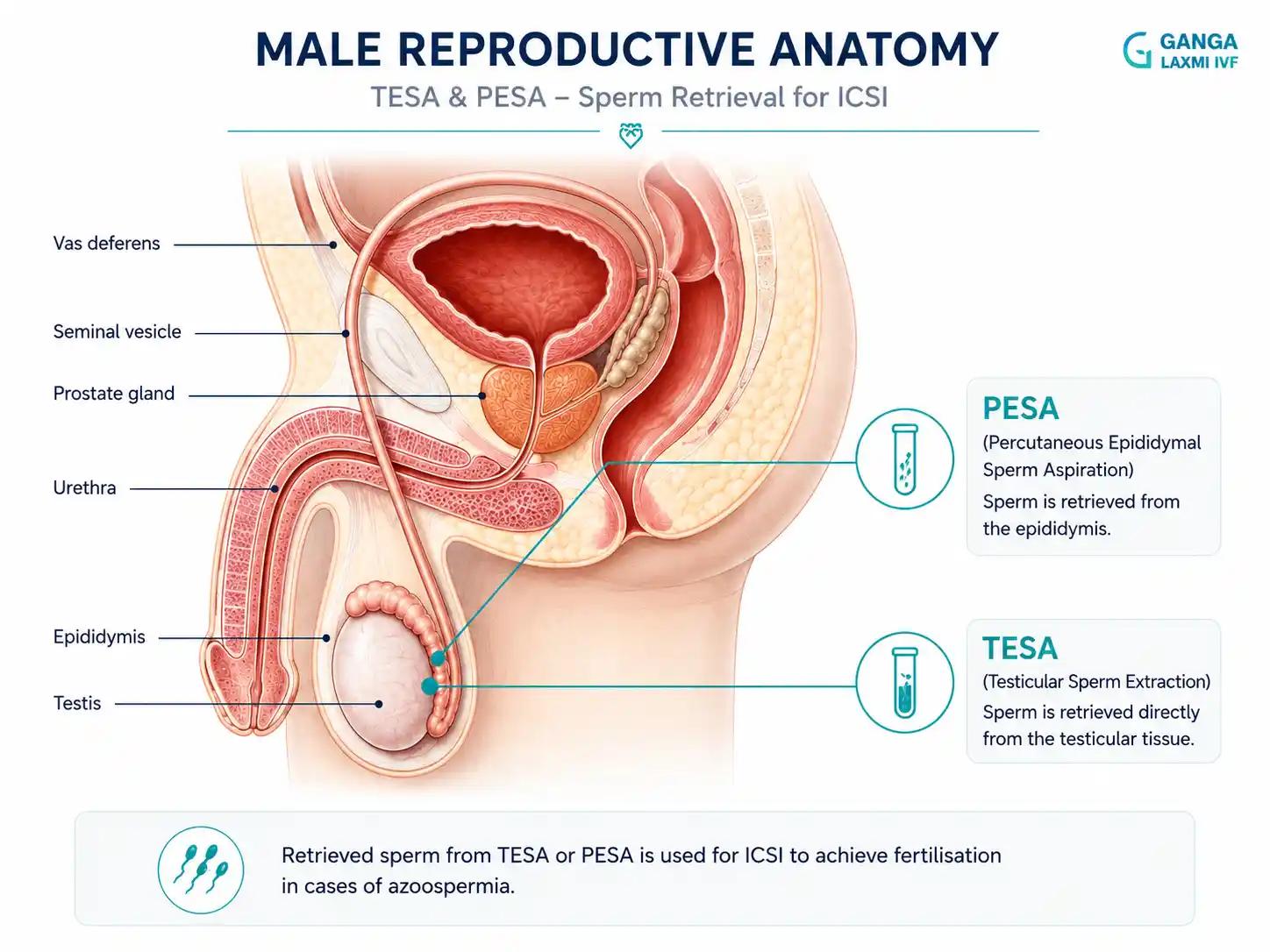
TESA and PESA: ICSI for Men with No Sperm in the Ejaculate
Azoospermia, the complete absence of sperm in the ejaculate, affects approximately 1 percent of all men and around 10 to 15 percent of men investigated for infertility. For many years this diagnosis meant that biological fatherhood was not possible.
TESA and PESA are surgical sperm retrieval procedures that, when combined with ICSI, have made fatherhood a realistic possibility for many men with azoospermia.
TESA
Full Name
Testicular Sperm Aspiration
How It Works
A fine needle is passed into the testicle under local anaesthesia to aspirate sperm directly from testicular tissue.
Who It Is For
Obstructive azoospermia (blockage preventing sperm release) and non-obstructive azoospermia where sperm production occurs only within the testis.
PESA
Full Name
Percutaneous Epididymal Sperm Aspiration
How It Works
A fine needle is inserted into the epididymis to retrieve sperm stored there.
Who It Is For
Obstructive azoospermia, including post-vasectomy patients or those with congenital absence of the vas deferens (CBAVD).
| Procedure | Full Name | How It Works | Who It Is For |
|---|---|---|---|
| TESA | Testicular Sperm Aspiration | A fine needle is passed into the testicle under local anaesthesia to aspirate sperm directly from testicular tissue. | Obstructive azoospermia (blockage preventing sperm release) and non-obstructive azoospermia where sperm production occurs only within the testis. |
| PESA | Percutaneous Epididymal Sperm Aspiration | A fine needle is inserted into the epididymis to retrieve sperm stored there. | Obstructive azoospermia, including post-vasectomy patients or those with congenital absence of the vas deferens (CBAVD). |
Two Types of Azoospermia and What They Mean for Treatment
Obstructive azoospermia means sperm are being produced normally in the testicles but cannot reach the ejaculate because of a blockage somewhere in the reproductive tract. This may be due to a prior vasectomy, congenital absence of the vas deferens (CBAVD, often associated with cystic fibrosis gene mutations), infection, or prior surgery. Sperm retrieval via TESA or PESA is highly successful in obstructive azoospermia.
Non-obstructive azoospermia means sperm production itself is impaired. However, even in non-obstructive azoospermia, small pockets of active sperm production may exist within the testicular tissue. Microsurgical TESA (microTESE) can identify and retrieve sperm from these areas. Success rates vary and depend on the underlying cause, but biological fatherhood remains achievable for many men with this diagnosis.
At Ganga Laxmi IVF, TESA and PESA procedures are coordinated with the IVF cycle so that retrieved sperm can be used fresh for ICSI on the same day as egg retrieval where possible. Dr. Chauhan manages the complete cycle from sperm retrieval through embryo transfer without the need for external referrals.
ICSI at Ganga Laxmi IVF, Lucknow
Male infertility is not a subject I approach with standard answers. Every man who comes to me has a different semen profile, a different history, and often a different level of anxiety about what the diagnosis means for him and his family. I take that seriously.
The consultation begins with a thorough semen analysis review, a complete medical and reproductive history, and where relevant, a physical examination or referral to a urologist or andrologist. Only once I have the full picture do I make a treatment recommendation.
ICSI only when clinically indicated
What It Means for You
Dr. Chauhan does not recommend ICSI routinely for every patient. It is prescribed only when your semen analysis, prior cycle history, or egg yield makes it the right choice. This protects you from unnecessary cost and intervention.
Semen analysis interpreted in full context
What It Means for You
A low count or motility reading alone does not determine your treatment. Dr. Chauhan reviews total motile sperm count, morphology, DNA fragmentation where indicated, and your partner's fertility parameters together before advising ICSI.
Experienced embryology team
What It Means for You
ICSI requires precision micromanipulation under high magnification. The skill of the embryologist directly affects fertilisation outcomes. Our embryology team performs ICSI with established, consistent protocols.
TESA and PESA available in-house
What It Means for You
Men with azoospermia do not need to be referred elsewhere for sperm retrieval. The procedure is coordinated with the IVF cycle on the same day so retrieved sperm are used fresh when possible.
Transparent cost discussion
What It Means for You
There are no hidden charges. ICSI pricing is discussed clearly before the cycle begins, alongside an honest assessment of your prognosis. Dr. Chauhan does not recommend procedures you do not need.
| What We Do | What It Means for You |
|---|---|
| ICSI only when clinically indicated | Dr. Chauhan does not recommend ICSI routinely for every patient. It is prescribed only when your semen analysis, prior cycle history, or egg yield makes it the right choice. This protects you from unnecessary cost and intervention. |
| Semen analysis interpreted in full context | A low count or motility reading alone does not determine your treatment. Dr. Chauhan reviews total motile sperm count, morphology, DNA fragmentation where indicated, and your partner's fertility parameters together before advising ICSI. |
| Experienced embryology team | ICSI requires precision micromanipulation under high magnification. The skill of the embryologist directly affects fertilisation outcomes. Our embryology team performs ICSI with established, consistent protocols. |
| TESA and PESA available in-house | Men with azoospermia do not need to be referred elsewhere for sperm retrieval. The procedure is coordinated with the IVF cycle on the same day so retrieved sperm are used fresh when possible. |
| Transparent cost discussion | There are no hidden charges. ICSI pricing is discussed clearly before the cycle begins, alongside an honest assessment of your prognosis. Dr. Chauhan does not recommend procedures you do not need. |
Confidential consultation
All consultations regarding male factor infertility at Ganga Laxmi IVF are completely confidential. Many men come to see Dr. Chauhan alone before involving their partner. This is entirely welcome. A clear, private conversation about your semen analysis results and your options is often the most useful first step.
Help centre
Frequently Asked Questions
These are the questions I am asked most often by men and couples who are considering ICSI. I have answered each one as I would in a consultation.
No. ICSI is more effective than standard IVF only when there is a specific reason for sperm to be unable to fertilise the egg on its own: low count, poor motility, abnormal morphology, azoospermia, or prior fertilisation failure. When sperm parameters are within normal range, standard IVF is equally effective and does not carry any disadvantage compared to ICSI. Recommending ICSI to every patient regardless of need is not sound clinical practice. Dr. Chauhan prescribes ICSI when the evidence supports it.
ICSI guarantees that fertilisation will be attempted with the best available sperm. Fertilisation itself is achieved in approximately 70 to 85 percent of injected mature eggs in well-conducted cycles. However, fertilisation is one step in a longer process. Whether a fertilised egg becomes a viable embryo, whether that embryo implants successfully, and whether the pregnancy continues all depend on additional factors including egg quality, embryo development, and uterine receptivity. Dr. Chauhan discusses realistic success rates for each individual based on age, ovarian reserve, sperm parameters, and prior cycle history before treatment begins.
This is an important and legitimate question. Men with severe oligospermia or non-obstructive azoospermia may carry genetic causes for their sperm production impairment, such as Y-chromosome microdeletions or chromosomal abnormalities. These can potentially be inherited by male children conceived through ICSI. For this reason, Dr. Chauhan recommends genetic counselling and karyotyping for men with severe male factor infertility before proceeding with ICSI. Where a hereditary genetic condition is identified, Preimplantation Genetic Testing (PGT) can be discussed as an additional option before embryo transfer.
ICSI is performed as part of a complete IVF cycle, with an additional laboratory charge for the microinjection procedure. The total cost depends on the medications used in your stimulation protocol, the number of eggs retrieved, and whether additional procedures such as TESA or sperm DNA fragmentation testing are required. Dr. Chauhan provides a complete, itemised cost estimate during the consultation before any cycle begins. There are no hidden charges. A first consultation to discuss your semen analysis and options is available for Rs. 400.
The ICSI microinjection itself is performed entirely in the embryology laboratory on retrieved eggs and sperm. Neither partner is present or involved in the injection step. For the woman, the experience is the same as a standard IVF cycle: stimulation injections, egg retrieval under sedation (a minor procedure completed in under 30 minutes), and embryo transfer, which is a simple, painless procedure similar to a smear test. For men who require TESA or PESA, the sperm retrieval is performed under local anaesthesia as a day procedure with minimal discomfort and a short recovery period. Most men return to normal activity within one to two days.
Male Infertility Is Treatable. You Do Not Have to Navigate It Alone.
A semen analysis result is a starting point, not a verdict. Whether your count is low, your motility is poor, or you have been told there are no sperm at all, ICSI has helped men in far more difficult situations than yours achieve fatherhood.
If you would like a clear, confidential, and honest assessment of your semen analysis and your options, I would like to help.
Confidential consultation
Book a confidential ICSI consultation
Low sperm count, poor motility, or azoospermia. Get a clear, private assessment of your semen analysis and options at Ganga Laxmi IVF, Gomti Nagar.
- Clinic
- 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow, 226010
- Hours
- Monday to Saturday, 9:00 AM to 8:00 PM
- Phone
- +91 72756 49692
- First consultation
- From Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
Male factor ICSI
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles
Male Infertility Treatment in Lucknow: Causes, Tests & Complete Guide
Male factors contribute to roughly half of all infertility cases. Dr. Kumudini Chauhan explains what causes male infertility, what a proper investigation looks like, and which treatments, from lifestyle changes to ICSI, are available at Ganga Laxmi IVF, Lucknow.

Laser Hatching and PGT After Failed IVF: Why Your Previous Cycles Failed and What to Do Next
Dr. Kumudini Chauhan explains why IVF fails, how Laser Assisted Hatching and PGT address those specific causes, and what a proper failed-IVF workup looks like at Ganga Laxmi IVF.

IVF After 40 in Lucknow: Advanced Age Fertility, PGT, and Realistic Hope
Fewer eggs, more chromosomal errors, harder decisions. Dr. Kumudini Chauhan explains what age actually does to your fertility, how PGT changes the odds, and what advanced age IVF looks like at Ganga Laxmi IVF, Lucknow.
PCOS and Pregnancy: Can You Conceive with PCOS?
Irregular cycles, no ovulation, conflicting advice. Dr. Kumudini Chauhan explains what PCOS actually does to your fertility, which treatments work at each stage, and what to expect at Ganga Laxmi IVF, Lucknow.