Of all the diagnoses I give in my clinic, unexplained infertility is the one that seems to leave patients the most unsettled. Not because it sounds serious, but because it does not sound like anything at all. Every test has come back normal. There is no blocked tube, no hormone problem, no obvious sperm issue. And yet, month after month, pregnancy has not happened.
The frustration this creates is real, and it is entirely understandable. You have done everything right. You have had the investigations. You have been patient. And the answer you received was, in effect, that medicine does not know exactly why it has not worked yet.
What I want to give you in this article is something more useful than a diagnosis: a clear, evidence-based treatment pathway. Where to start, what to expect, when to move forward, and why. Unexplained infertility is treatable. Most couples who pursue treatment systematically do achieve pregnancy. The question is simply which step to take next, and when.
Key statistic
Unexplained infertility accounts for approximately 15 to 25 percent of all infertility investigations, making it one of the most common fertility diagnoses.
The majority of couples with unexplained infertility who receive appropriate treatment go on to achieve pregnancy.
What Is Unexplained Infertility?
Unexplained infertility is a clinical diagnosis of exclusion. It is reached when a couple has been trying to conceive for twelve months or more (or six months if the woman is over 35) and a standard fertility workup returns results within accepted normal ranges across all key parameters.
This does not mean nothing is wrong. It means the current standard investigations have not detected a specific abnormality. Fertilisation may be failing at a subtle biological level that is not visible in a routine semen analysis or ultrasound. Egg-sperm interaction, sperm DNA integrity, early embryo development, or implantation mechanisms may all be contributing to the problem without appearing abnormal on paper.
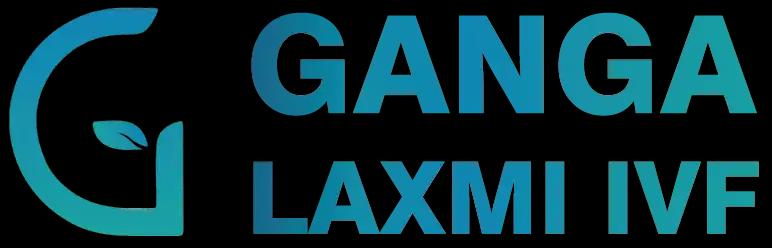
Standard Investigations That Must All Be Normal for This Diagnosis
Semen Analysis (WHO 2021)
What Is Assessed
Sperm count, motility, morphology, volume, pH.
Result in Unexplained Infertility
Within normal reference limits.
Ovulation Confirmation
What Is Assessed
Day 2/3 FSH, LH, AMH, antral follicle count; mid-luteal progesterone.
Result in Unexplained Infertility
Ovulation occurring; hormone levels within expected range.
Tubal Patency Testing (HSG)
What Is Assessed
Whether fallopian tubes are open and functional.
Result in Unexplained Infertility
Both tubes open with no obstruction.
Uterine Assessment
What Is Assessed
Ultrasound and/or hysteroscopy to evaluate uterine cavity.
Result in Unexplained Infertility
No polyps, fibroids, septum, or adhesions detected.
Thyroid Function (TSH)
What Is Assessed
Thyroid status, which directly affects ovulation and implantation.
Result in Unexplained Infertility
Within normal range.
Prolactin
What Is Assessed
Elevated prolactin can suppress ovulation and implantation.
Result in Unexplained Infertility
Normal.
Postcoital Test (selected cases)
What Is Assessed
Interaction of sperm and cervical mucus.
Result in Unexplained Infertility
Normal sperm survival in cervical mucus. (Less commonly used now.)
| Investigation | What Is Assessed | Result in Unexplained Infertility |
|---|---|---|
| Semen Analysis (WHO 2021) | Sperm count, motility, morphology, volume, pH. | Within normal reference limits. |
| Ovulation Confirmation | Day 2/3 FSH, LH, AMH, antral follicle count; mid-luteal progesterone. | Ovulation occurring; hormone levels within expected range. |
| Tubal Patency Testing (HSG) | Whether fallopian tubes are open and functional. | Both tubes open with no obstruction. |
| Uterine Assessment | Ultrasound and/or hysteroscopy to evaluate uterine cavity. | No polyps, fibroids, septum, or adhesions detected. |
| Thyroid Function (TSH) | Thyroid status, which directly affects ovulation and implantation. | Within normal range. |
| Prolactin | Elevated prolactin can suppress ovulation and implantation. | Normal. |
| Postcoital Test (selected cases) | Interaction of sperm and cervical mucus. | Normal sperm survival in cervical mucus. (Less commonly used now.) |
If your results meet the above criteria and you have been trying for the appropriate duration, unexplained infertility is the correct working diagnosis. The treatment approach described in this article is designed specifically for you.
Why IUI Is the Right First Step for Unexplained Infertility
When all investigations are normal, the treatment principle is straightforward: start with the least invasive, most cost-effective option that meaningfully improves the chance of pregnancy, and escalate only if it does not succeed within a reasonable number of attempts.
For unexplained infertility, that first step isIUI Treatment in Lucknow, or Intrauterine Insemination.
IUI works by shortening the distance sperm must travel to reach the egg. In natural conception, sperm deposited in the vagina must navigate through the cervix, across the uterine cavity, and into the fallopian tube where the egg is waiting. Many do not make it. IUI places washed, concentrated sperm directly inside the uterine cavity, giving them a significantly shorter and more direct route to the egg.
This is combined with carefully timed ovulation monitoring so that insemination occurs within the optimal fertilisation window. In many unexplained infertility cases, IUI with ovarian stimulation is enough to tip the balance in favour of conception.
How the IUI Process Works at Ganga Laxmi IVF
Step 1 — Cycle Monitoring
Stage
Cycle Monitoring
What Happens
From Day 2 of the menstrual cycle, ultrasound scans track follicle development. Mild stimulation with oral medications (clomiphene citrate or letrozole) or low-dose gonadotrophins is often used to encourage one to two dominant follicles.
Step 2 — Trigger Injection
Stage
Trigger Injection
What Happens
When the dominant follicle reaches 18 to 20mm, an hCG or GnRH agonist trigger injection is given to time ovulation precisely. IUI is scheduled 36 to 40 hours after the trigger.
Step 3 — Semen Collection and Sperm Washing
Stage
Semen Collection and Sperm Washing
What Happens
A semen sample is produced on the day of IUI. Laboratory processing concentrates the motile sperm fraction and removes seminal plasma, which could cause uterine cramping if introduced directly.
Step 4 — Insemination
Stage
Insemination
What Happens
A soft, flexible catheter is passed through the cervix into the uterine cavity. The washed sperm sample is gently deposited directly at the top of the uterus.
Step 5 — Luteal Phase Support
Stage
Luteal Phase Support
What Happens
Progesterone pessaries or gel are usually prescribed from Day 3 after IUI to support the uterine lining in case fertilisation and implantation occur.
Step 6 — Pregnancy Test
Stage
Pregnancy Test
What Happens
A urine or blood beta-hCG test is done approximately 14 to 16 days after IUI. A blood test is more sensitive and gives an earlier, more reliable result.
| Step | Stage | What Happens |
|---|---|---|
| 1 | Cycle Monitoring | From Day 2 of the menstrual cycle, ultrasound scans track follicle development. Mild stimulation with oral medications (clomiphene citrate or letrozole) or low-dose gonadotrophins is often used to encourage one to two dominant follicles. |
| 2 | Trigger Injection | When the dominant follicle reaches 18 to 20mm, an hCG or GnRH agonist trigger injection is given to time ovulation precisely. IUI is scheduled 36 to 40 hours after the trigger. |
| 3 | Semen Collection and Sperm Washing | A semen sample is produced on the day of IUI. Laboratory processing concentrates the motile sperm fraction and removes seminal plasma, which could cause uterine cramping if introduced directly. |
| 4 | Insemination | A soft, flexible catheter is passed through the cervix into the uterine cavity. The washed sperm sample is gently deposited directly at the top of the uterus. |
| 5 | Luteal Phase Support | Progesterone pessaries or gel are usually prescribed from Day 3 after IUI to support the uterine lining in case fertilisation and implantation occur. |
| 6 | Pregnancy Test | A urine or blood beta-hCG test is done approximately 14 to 16 days after IUI. A blood test is more sensitive and gives an earlier, more reliable result. |
Why IUI Makes Sense as a First Step
- IUI is an outpatient procedure. No anaesthesia, no egg retrieval, no laboratory fertilisation.
- It is significantly less expensive than IVF and does not require the physical and emotional commitment of a full IVF cycle.
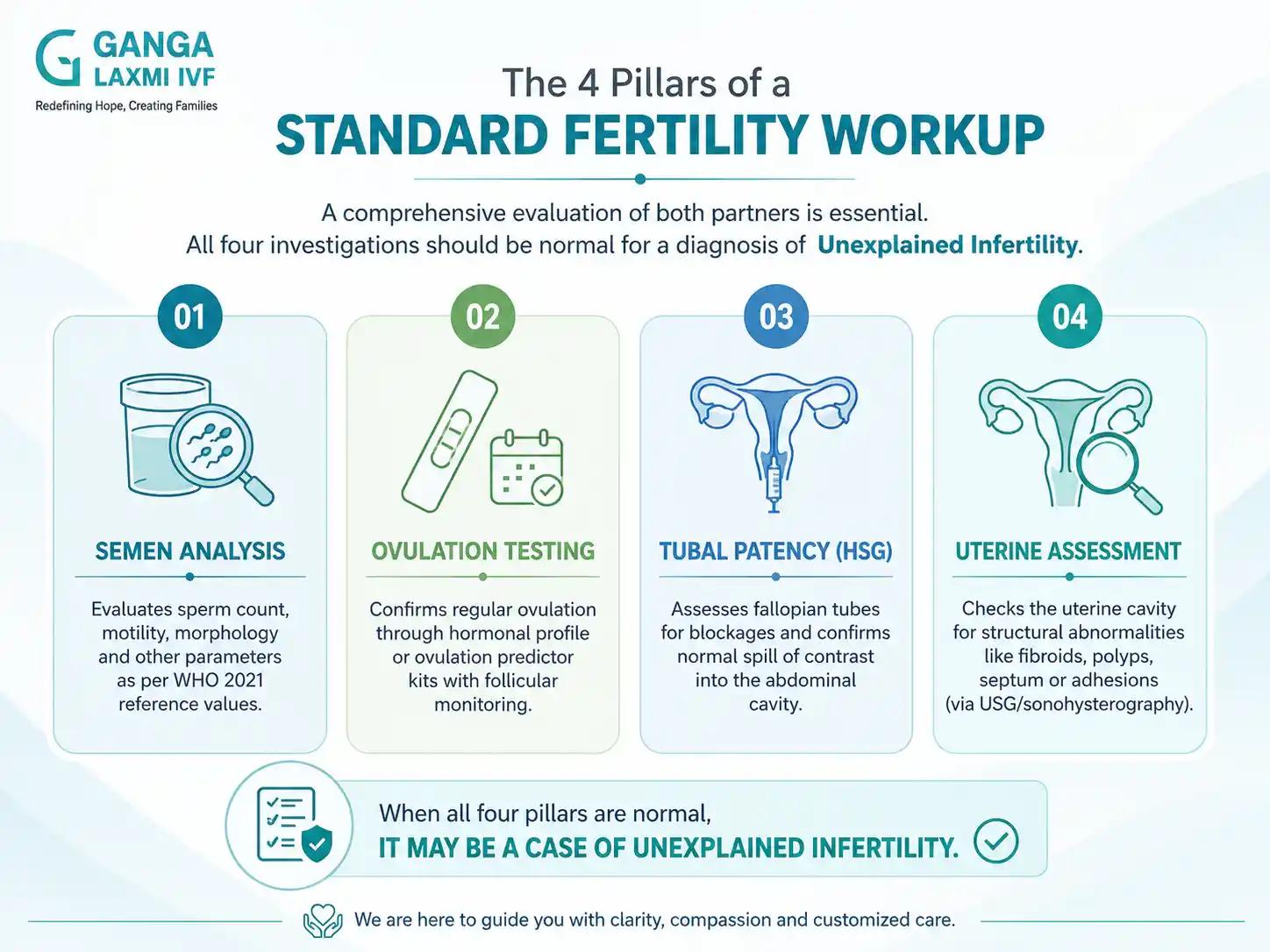
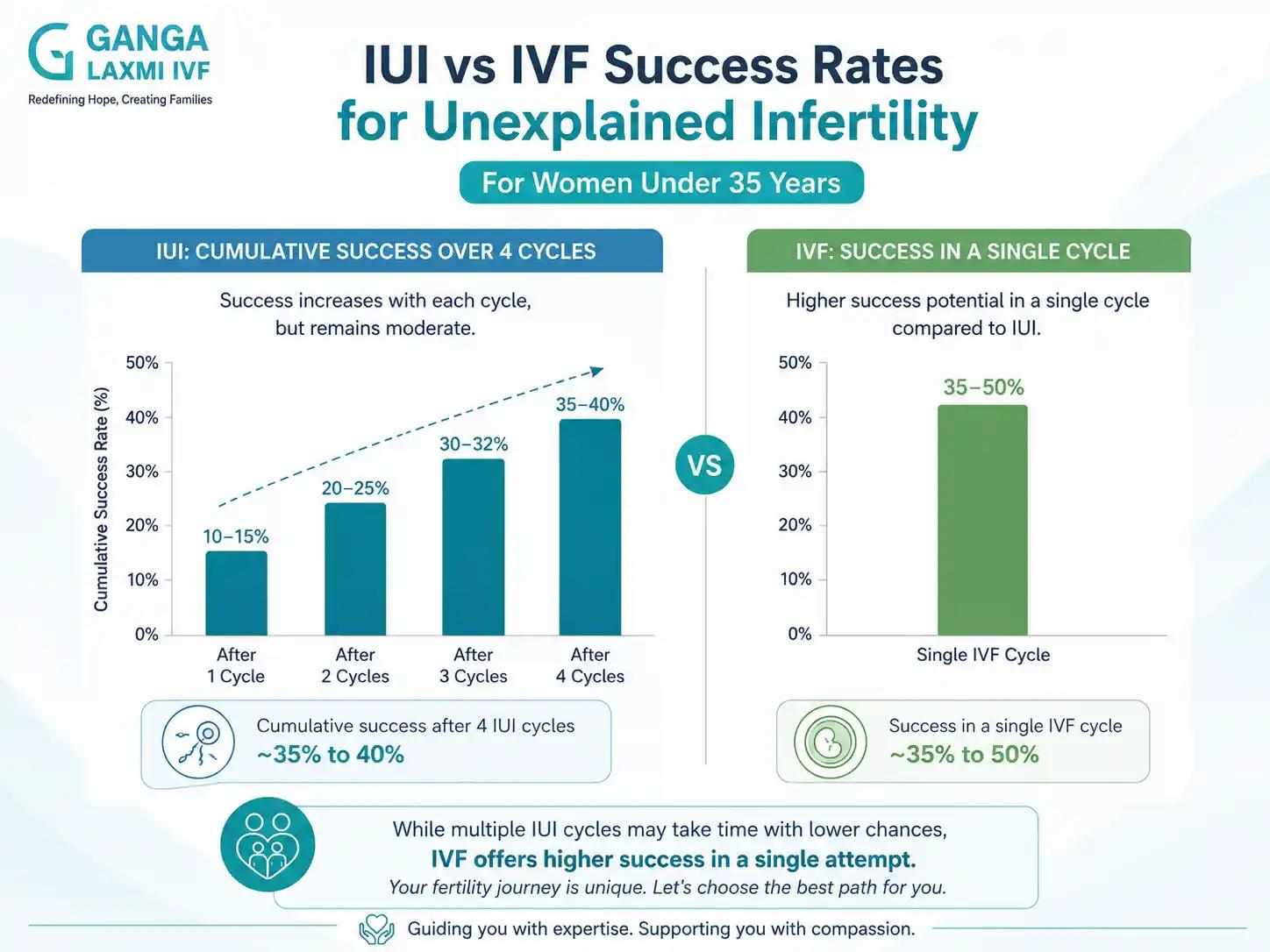
- When tubes are open, sperm parameters are adequate, and the woman is under 35, IUI with stimulation gives a reasonable per-cycle success rate of approximately 10 to 15 percent for unexplained infertility. Over three to four cycles, the cumulative success rate reaches approximately 30 to 40 percent.
- At Ganga Laxmi IVF, we do not recommend IVF when IUI is clinically appropriate. We always begin at the step that is right for you, not the step that is most expensive.
IUI Treatment in Lucknow: Who Is the Ideal Candidate?
Not every couple with unexplained infertility is at the same stage of their fertility journey, and not every couple is the right candidate for IUI at the same time. When I see a new patient at Ganga Laxmi IVF, I review the full investigation picture before recommending IUI. As a fertility specialist in Lucknow treating unexplained infertility for over two decades, my starting point is always the same question: what is the least invasive treatment that gives this couple a meaningful chance of pregnancy right now?
IUI is the right first step when the following conditions are met:
- Both fallopian tubes are open and confirmed patent on HSG (hysterosalpingography)
- Sperm count and motility are within acceptable parameters on semen analysis (WHO 2021 reference values)
- Ovulation is occurring or can be induced with mild oral stimulation (clomiphene citrate or letrozole)
- The woman is under 35, or between 35 and 37 with a reassuring ovarian reserve
- There is no prior history of failed fertilisation in an IVF cycle
When these conditions are present, there is no clinical reason to move directly to IVF. IUI with ovarian stimulation gives a per-cycle success rate of approximately 10 to 15 percent for unexplained infertility. Across three to four cycles, the cumulative success rate reaches 30 to 40 percent, which is a meaningful chance of pregnancy without the physical and financial commitment of a full IVF cycle.
Couples who do not meet these criteria — for example, those with borderline sperm parameters, reduced ovarian reserve, or age above 38, may be better served by moving directly to IVF. As your IUI doctor in Lucknow, I give each couple a personalised assessment before any treatment is recommended. The goal is always to match the treatment to your specific situation, not to apply a standard protocol.
Candidate Suitability at a Glance
Tubal patency
Suitable for IUI
Both tubes open on HSG
Consider Moving to IVF
One or both tubes blocked
Sperm parameters
Suitable for IUI
Within WHO 2021 normal range
Consider Moving to IVF
Borderline or worsening counts
Female age
Suitable for IUI
Under 35 (or 35–37 with good reserve)
Consider Moving to IVF
38 and above
Ovarian reserve (AMH)
Suitable for IUI
Within expected range for age
Consider Moving to IVF
Low AMH or poor antral follicle count
Prior IVF history
Suitable for IUI
No previous IVF attempted
Consider Moving to IVF
Failed fertilisation in a previous IVF cycle
Cycle count
Suitable for IUI
Fewer than 3–4 IUI attempts
Consider Moving to IVF
3 or more failed IUI cycles
| Clinical Factor | Suitable for IUI | Consider Moving to IVF |
|---|---|---|
| Tubal patency | Both tubes open on HSG | One or both tubes blocked |
| Sperm parameters | Within WHO 2021 normal range | Borderline or worsening counts |
| Female age | Under 35 (or 35–37 with good reserve) | 38 and above |
| Ovarian reserve (AMH) | Within expected range for age | Low AMH or poor antral follicle count |
| Prior IVF history | No previous IVF attempted | Failed fertilisation in a previous IVF cycle |
| Cycle count | Fewer than 3–4 IUI attempts | 3 or more failed IUI cycles |
This table provides a general framework. Individual clinical factors always take precedence. If you are unsure whether IUI or IVF is the right step for you, a consultation with a qualified IUI specialist in Lucknow is the most reliable way to get a clear answer based on your own investigation results.
What Is the Cost of IUI Treatment in Lucknow?
Cost is a practical consideration for every couple, and I believe in giving patients a clear and honest picture before they commit to any treatment. IUI is significantly more affordable than IVF, which is one of the reasons it is the clinically appropriate first step for most couples with unexplained infertility.
In Lucknow, the cost of a single IUI cycle typically ranges from ₹8,000 to ₹18,000, depending on the medications used, the number of monitoring ultrasounds required, and whether the cycle includes mild ovarian stimulation. The variation in cost reflects the clinical needs of each patient. Not all cycles require the same level of monitoring or the same medication protocols.
The following table outlines the components that typically contribute to the total cost of an IUI cycle:
Consultation and assessment
Details
Initial review of investigations and cycle planning
Ovarian stimulation medication
Details
Oral agents (clomiphene or letrozole) are lower cost; injectable gonadotrophins are used when indicated and cost more
Follicle monitoring ultrasounds
Details
Typically 2 to 3 scans per cycle to track follicle growth
Trigger injection (hCG or GnRH agonist)
Details
Used to time ovulation precisely before insemination
Semen analysis and sperm washing
Details
Laboratory processing of the sample on the day of IUI
Insemination procedure
Details
The IUI procedure itself (outpatient, no anaesthesia required)
Luteal phase progesterone support
Details
Pessaries or gel prescribed from Day 3 post-IUI
Pregnancy test (blood beta-hCG)
Details
Conducted approximately 14 to 16 days after IUI
| Cost Component | Details |
|---|---|
| Consultation and assessment | Initial review of investigations and cycle planning |
| Ovarian stimulation medication | Oral agents (clomiphene or letrozole) are lower cost; injectable gonadotrophins are used when indicated and cost more |
| Follicle monitoring ultrasounds | Typically 2 to 3 scans per cycle to track follicle growth |
| Trigger injection (hCG or GnRH agonist) | Used to time ovulation precisely before insemination |
| Semen analysis and sperm washing | Laboratory processing of the sample on the day of IUI |
| Insemination procedure | The IUI procedure itself (outpatient, no anaesthesia required) |
| Luteal phase progesterone support | Pessaries or gel prescribed from Day 3 post-IUI |
| Pregnancy test (blood beta-hCG) | Conducted approximately 14 to 16 days after IUI |
Before your first cycle, you will receive a clear breakdown of all expected costs so there are no surprises. If your treatment plan changes at any point (for example, if a monitoring scan shows the need for an additional injection), I will explain the reason and the cost implication before proceeding.
When you compare the cost of three to four IUI cycles against a single IVF cycle, IUI remains the more cost-effective pathway for couples who are clinically suitable. If IUI does not succeed within the appropriate number of cycles, moving to IVF is the evidence-based next step, and the information gained from each IUI cycle helps refine your IVF plan.
How Many IUI Cycles Before Moving to IVF?
This is the question I am asked most often by patients who have had one or two unsuccessful IUI cycles and are wondering whether to continue or move forward. The answer is not the same for every patient, and I will not pretend it is. But the clinical evidence gives us a clear general framework.
The cumulative success of IUI improves meaningfully with each cycle up to approximately three to four attempts. Beyond four cycles in unexplained infertility, the per-cycle success rate does not increase further, and the cumulative advantage over IVF begins to diminish significantly. Continuing IUI past this point generally adds delay without adding meaningful benefit.
When to Escalate: Decision Guide by Patient Situation
Under 35, all tests normal, 3 failed IUI cycles
Recommended Action
Consider IVF after cycle 3.
Why
Per-cycle success of IVF significantly exceeds IUI in unexplained cases from cycle 4 onwards.
Under 35, all tests normal, 4 failed IUI cycles
Recommended Action
Move to IVF.
Why
Continuing IUI beyond 4 cycles adds delay without meaningful improvement in cumulative success.
Age 35 to 37
Recommended Action
Consider IVF after 2 to 3 IUI cycles.
Why
Egg quality begins to decline in the mid-thirties. Earlier escalation preserves better embryos.
Age 38 or above
Recommended Action
Discuss IVF from the outset or after 1 to 2 IUI cycles.
Why
Ovarian reserve and egg quality decline accelerates. Time is a real clinical factor from this age.
Sperm parameters borderline or worsening
Recommended Action
Move to IVF with ICSI consideration earlier.
Why
IUI depends on sufficient motile sperm reaching the tubes. Declining parameters reduce IUI efficacy further.
Significant emotional distress or time pressure
Recommended Action
Discuss moving to IVF sooner.
Why
Patient wellbeing is a legitimate clinical consideration. Dr. Chauhan does not require you to complete a fixed number of IUI cycles if you are not able to sustain more.
Any failed fertilisation in a previous IVF cycle
Recommended Action
Move to IVF with ICSI.
Why
Failed fertilisation in standard IVF confirms a fertilisation barrier that only ICSI can resolve.
| Situation | Recommended Action | Why |
|---|---|---|
| Under 35, all tests normal, 3 failed IUI cycles | Consider IVF after cycle 3. | Per-cycle success of IVF significantly exceeds IUI in unexplained cases from cycle 4 onwards. |
| Under 35, all tests normal, 4 failed IUI cycles | Move to IVF. | Continuing IUI beyond 4 cycles adds delay without meaningful improvement in cumulative success. |
| Age 35 to 37 | Consider IVF after 2 to 3 IUI cycles. | Egg quality begins to decline in the mid-thirties. Earlier escalation preserves better embryos. |
| Age 38 or above | Discuss IVF from the outset or after 1 to 2 IUI cycles. | Ovarian reserve and egg quality decline accelerates. Time is a real clinical factor from this age. |
| Sperm parameters borderline or worsening | Move to IVF with ICSI consideration earlier. | IUI depends on sufficient motile sperm reaching the tubes. Declining parameters reduce IUI efficacy further. |
| Significant emotional distress or time pressure | Discuss moving to IVF sooner. | Patient wellbeing is a legitimate clinical consideration. Dr. Chauhan does not require you to complete a fixed number of IUI cycles if you are not able to sustain more. |
| Any failed fertilisation in a previous IVF cycle | Move to IVF with ICSI. | Failed fertilisation in standard IVF confirms a fertilisation barrier that only ICSI can resolve. |
There is no rule that requires you to complete a fixed number of IUI cycles before discussing IVF. If your circumstances, age, or emotional wellbeing make an earlier transition to IVF the right choice, that conversation is always available to you.
IVF After Failed IUIs: When to Make the Move
When three to four IUI cycles have not resulted in pregnancy, IVF is the natural and well-evidenced next step. The reason is not simply that IVF is a more powerful version of IUI. They work in fundamentally different ways.
IUI improves the quantity and positioning of sperm in relation to the egg. It still depends on fertilisation happening inside the body, and it cannot identify or correct whatever subtle barrier may be preventing that from happening.
IVF removes the barrier entirely. Eggs are retrieved directly from the ovaries. Sperm and eggs are brought together in a controlled laboratory environment. The fertilisation process is observed in real time. If fertilisation occurs and a healthy embryo develops, it is transferred directly into the uterus.
IUI vs IVF for Unexplained Infertility: A Direct Comparison
What it does
IUI
Brings washed sperm closer to the egg. Fertilisation still happens inside the body.
IVF
Retrieves eggs from the ovary and fertilises them in the laboratory under controlled conditions.
Per-cycle success rate (unexplained infertility, under 35)
IUI
Approximately 10 to 15% per cycle.
IVF
Approximately 35 to 50% per cycle, depending on age and ovarian reserve.
Invasiveness
IUI
Minimal. Outpatient procedure. No anaesthesia.
IVF
Moderate. Egg retrieval under sedation. Stimulation injections over 10 to 12 days.
Cost
IUI
Significantly lower than IVF.
IVF
Higher. Includes laboratory, embryology, and medication costs.
What it cannot fix
IUI
Cannot overcome fertilisation failure, subtle egg-sperm interaction problems, or poor egg quality.
IVF
Addresses fertilisation directly. Can identify and resolve fertilisation failure. ICSI available if needed.
Who it suits best
IUI
Open tubes, acceptable sperm, younger patients, early in the treatment journey.
IVF
After failed IUI cycles; older patients; where a fertilisation barrier is suspected; when time is a factor.
| Factor | IUI | IVF |
|---|---|---|
| What it does | Brings washed sperm closer to the egg. Fertilisation still happens inside the body. | Retrieves eggs from the ovary and fertilises them in the laboratory under controlled conditions. |
| Per-cycle success rate (unexplained infertility, under 35) | Approximately 10 to 15% per cycle. | Approximately 35 to 50% per cycle, depending on age and ovarian reserve. |
| Invasiveness | Minimal. Outpatient procedure. No anaesthesia. | Moderate. Egg retrieval under sedation. Stimulation injections over 10 to 12 days. |
| Cost | Significantly lower than IVF. | Higher. Includes laboratory, embryology, and medication costs. |
| What it cannot fix | Cannot overcome fertilisation failure, subtle egg-sperm interaction problems, or poor egg quality. | Addresses fertilisation directly. Can identify and resolve fertilisation failure. ICSI available if needed. |
| Who it suits best | Open tubes, acceptable sperm, younger patients, early in the treatment journey. | After failed IUI cycles; older patients; where a fertilisation barrier is suspected; when time is a factor. |
There is one particularly important insight that IVF provides that IUI cannot: information. When fertilisation fails in a standard IVF cycle, you learn something critical. You learn that there is a fertilisation barrier, not just an unexplained absence of pregnancy. That information changes the treatment plan and points directly toward ICSI as the solution.
This is why I sometimes refer to IVF, for unexplained infertility patients who have failed multiple IUI cycles, as both a treatment and a diagnostic step. It tells us whether fertilisation can happen naturally in ideal laboratory conditions, and if not, it tells us what to do next.
A note on per-cycle success rates
The success rates quoted for IVF and IUI reflect published literature for patients with unexplained infertility under 35 with good ovarian reserve. Individual rates depend on age, AMH, antral follicle count, sperm parameters, and prior cycle history.
Dr. Chauhan provides personalised success estimates based on your specific investigations before recommending any treatment. Published averages are useful for planning, but your individual picture is what actually determines your prognosis.
ICSI in Unexplained Infertility: When IVF Alone Is Not Enough
For a subset of unexplained infertility patients, a standard IVF cycle retrieves eggs and sperm is prepared, but fertilisation does not occur or is very poor. This is called unexplained fertilisation failure, and it is only identifiable once an IVF cycle is attempted.
In this situation, ICSI is the solution. By injecting a single sperm directly into each mature egg, ICSI bypasses whatever biological mechanism was preventing fertilisation. The majority of patients who experience fertilisation failure in standard IVF achieve normal fertilisation rates when the same cycle is repeated with ICSI.
The Full Treatment Pathway for Unexplained Infertility
Step 1 — IUI
Treatment
IUI
Per-Cycle Success*
10 to 15%
When to Use
All standard tests normal; open tubes; adequate sperm; patient under 35.
When to Move Forward
After 3 to 4 failed cycles, or earlier if age is over 35.
Step 2 — IVF
Treatment
IVF
Per-Cycle Success*
35 to 50%
When to Use
After failed IUI cycles; or first-line for age 38+, poor ovarian reserve, or borderline sperm.
When to Move Forward
If fertilisation fails in standard IVF, or embryo quality is persistently poor.
Step 3 — IVF + ICSI
Treatment
IVF + ICSI
Per-Cycle Success*
35 to 50%
When to Use
When IVF fertilisation has failed; severe male factor confirmed; or per Dr. Chauhan's recommendation.
When to Move Forward
Success at this stage addresses most unexplained infertility causes.
| Step | Treatment | Per-Cycle Success* | When to Use | When to Move Forward |
|---|---|---|---|---|
| 1 | IUI | 10 to 15% | All standard tests normal; open tubes; adequate sperm; patient under 35. | After 3 to 4 failed cycles, or earlier if age is over 35. |
| 2 | IVF | 35 to 50% | After failed IUI cycles; or first-line for age 38+, poor ovarian reserve, or borderline sperm. | If fertilisation fails in standard IVF, or embryo quality is persistently poor. |
| 3 | IVF + ICSI | 35 to 50% | When IVF fertilisation has failed; severe male factor confirmed; or per Dr. Chauhan's recommendation. | Success at this stage addresses most unexplained infertility causes. |
* Success rates are approximate per-cycle figures for women under 35 with unexplained infertility and good ovarian reserve. Individual rates vary. Source: published NICE guidelines and HFEA registry data.
ICSI for unexplained infertility is covered in greater detail in our companion article on ICSI and male infertility. If you have been through IUI cycles and one or more IVF cycles without fertilisation, that article is worth reading before your next consultation.

Dr. Kumudini Chauhan's Approach to Unexplained Infertility
I have been treating unexplained infertility in Lucknow for twenty years. It remains one of the most nuanced areas of fertility medicine, precisely because there is no single obvious target to treat.
My approach is built on one principle above all others: the right treatment for you is the least invasive option that still gives you a meaningful chance of success at this stage of your journey. I do not recommend IVF when IUI is appropriate. I do not recommend ICSI when standard IVF is appropriate. And I do not keep patients in IUI cycles beyond the point where continuing makes clinical sense.
What this looks like in practice: I review your complete investigations, your age, your partner's semen parameters, how many cycles you have already attempted, and how you are feeling emotionally and physically. I then give you a clear recommendation with an honest explanation of why.
Unexplained infertility does not mean untreatable infertility. It means we have not yet found the precise step that unlocks your cycle. In my experience, with a methodical approach and the right escalation at the right time, most couples find that step.
Dr. Chauhan's Principle
Start with the least invasive step
What It Means for You
IUI is recommended first when it is clinically appropriate. No couple is pushed to IVF before IUI has been given a fair chance.
Escalate at the right time, not too early and not too late
What It Means for You
Dr. Chauhan follows evidence-based escalation criteria while accounting for your individual age, reserve, and emotional state.
Every cycle generates information
What It Means for You
Even a failed IUI or IVF cycle tells us something. Dr. Chauhan reviews each cycle outcome before planning the next step.
You will never be kept in a loop
What It Means for You
If continuing the same treatment is no longer the right clinical decision, Dr. Chauhan will tell you clearly and explain why escalation is now appropriate.
Personalised success estimates before every cycle
What It Means for You
Before you commit to any treatment, you receive an honest, individualised assessment of your likely outcomes based on your specific investigations.
| Principle | What It Means for You |
|---|---|
| Start with the least invasive step | IUI is recommended first when it is clinically appropriate. No couple is pushed to IVF before IUI has been given a fair chance. |
| Escalate at the right time, not too early and not too late | Dr. Chauhan follows evidence-based escalation criteria while accounting for your individual age, reserve, and emotional state. |
| Every cycle generates information | Even a failed IUI or IVF cycle tells us something. Dr. Chauhan reviews each cycle outcome before planning the next step. |
| You will never be kept in a loop | If continuing the same treatment is no longer the right clinical decision, Dr. Chauhan will tell you clearly and explain why escalation is now appropriate. |
| Personalised success estimates before every cycle | Before you commit to any treatment, you receive an honest, individualised assessment of your likely outcomes based on your specific investigations. |
Why Couples in Lucknow Choose IUI First
Every week, I meet couples at Ganga Laxmi IVF who have spent months looking for a clear answer to one question: where do we start? Many of them have already done their investigations. The semen analysis is normal. The tubes are open. Ovulation is happening. And yet, pregnancy has not occurred.
These couples come from across Lucknow: from Gomti Nagar and Indira Nagar, from Aliganj and Hazratganj, from Alambagh and Mahanagar, and from neighbouring towns in Uttar Pradesh including Unnao, Rae Bareli, and Sitapur. What they share is a diagnosis of unexplained infertility and a need for a clear, sensible next step.
For the majority of these couples, that next step is IUI.
There are practical reasons why IUI is the treatment most couples in Lucknow begin with, and they go beyond cost.
- IUI is an outpatient procedure. There is no hospitalisation, no egg retrieval, and no general anaesthesia. Most couples are able to return to work the same day.
- IUI fits around a working couple's schedule. With precise ovulation timing, the insemination window is planned in advance. This matters for couples where one or both partners work full-time or have long commutes.
- IUI gives the body a structured, supported chance to conceive naturally. For couples with unexplained infertility where no specific barrier has been identified, this is clinically sound — it addresses the most likely obstacles around sperm transport and fertilisation timing, without bypassing the natural process entirely.
- IUI generates useful information. If IUI does not succeed, the pattern of response guides the next step. It helps identify whether the issue is likely to involve fertilisation, which then informs the IVF approach.
Many couples from Gomti Nagar and surrounding areas of Lucknow are advised to begin with IUI before considering IVF, particularly when they meet the standard candidacy criteria: open tubes, acceptable sperm parameters, female age under 35, and no prior IVF history. This is not a delay. It is the right clinical starting point.
At Ganga Laxmi IVF in Gomti Nagar, I do not recommend IVF when IUI is appropriate. I also do not keep couples in IUI cycles past the point where continuing makes clinical sense. The goal is always a pregnancy, reached by the most direct, appropriate path for your specific situation.
Help centre
Frequently Asked Questions
These are the questions I hear most often from patients who have received a diagnosis of unexplained infertility. I have answered each one as I would in a consultation.
In some cases, yes. Studies suggest that around 25 to 30 percent of couples diagnosed with unexplained infertility conceive naturally within two years without treatment, particularly younger couples where the investigation has been thorough and reassuring. This is why clinical guidelines do not automatically recommend immediate treatment in all cases. However, for couples where the woman is over 35, or where the emotional and practical toll of waiting has been significant, or where repeated natural cycles have already been attempted, watchful waiting is rarely the right approach. Dr. Chauhan will always give you an honest view of whether natural conception is a realistic expectation in your specific situation.
For most patients under 35 with unexplained infertility and no other complicating factors, the evidence supports attempting three to four IUI cycles before moving to IVF. This is because the cumulative success of IUI improves over this range, and three to four cycles gives the treatment a fair trial without unnecessary delay. For women aged 35 to 37, two to three cycles is a more appropriate threshold. For women over 38, the conversation about moving directly to IVF from the outset, or after one to two IUI cycles, is entirely justified because ovarian reserve and egg quality decline meaningfully in this age range. There is no rule that applies to every patient, and Dr. Chauhan reviews this with you individually.
No. Many patients with unexplained infertility conceive during IUI cycles, and a proportion conceive naturally with close monitoring and cycle optimisation. IVF becomes necessary when IUI has not succeeded after the appropriate number of cycles, when age or ovarian reserve makes a faster escalation clinically appropriate, or when fertilisation failure in IVF points to a specific barrier that only ICSI can address. Dr. Chauhan does not recommend IVF as a first step unless the clinical situation specifically warrants it.
This question deserves an honest answer, because stress is frequently cited as a cause of infertility in ways that are not well supported by evidence and can be genuinely harmful to patients who are already struggling. Severe, chronic stress can affect hormone levels and disrupt ovulation in some cases. But for the vast majority of couples with unexplained infertility, stress is not the underlying cause. The biological mechanisms that fertility treatment addresses, such as subtle fertilisation failure, sperm-egg interaction, or embryo quality, are not resolved by stress reduction alone. I say this not to dismiss the importance of emotional wellbeing, which genuinely matters and which I take seriously, but to make clear that unexplained infertility is a medical situation that deserves a medical response, not an instruction to relax and try again.
If you have a diagnosis of unexplained infertility, the standard workup should include: a full semen analysis interpreted against WHO 2021 reference values; hormone testing including FSH, LH, AMH, and prolactin on Day 2 or 3; mid-luteal progesterone to confirm ovulation; thyroid function (TSH); a hysterosalpingogram (HSG) to confirm tubal patency; and baseline ultrasound assessment of antral follicle count and uterine cavity. If these have already been done and all are normal, the next step is not more testing but treatment. Some couples request additional investigations such as sperm DNA fragmentation, endometrial receptivity assessment, or immune testing. Dr. Chauhan will advise which of these are relevant to your situation and which are not likely to change the treatment plan.
For couples with unexplained infertility, IUI success rates are typically 10–15% per cycle. After 3–4 cycles, cumulative success rates may reach 30–40%, especially in women under 35.
The cost of an IUI cycle in Lucknow varies depending on medications, monitoring, and laboratory procedures. A personalized cost estimate can be provided after a fertility consultation and treatment assessment.
Choose an experienced fertility specialist who offers evidence-based treatment recommendations. Dr. Kumudini Chauhan, a senior infertility specialist in Lucknow with over 20 years of experience, provides personalized IUI and IVF treatment planning.
Yes. IUI can still be effective after 2 years of unexplained infertility if fertility tests are normal and there are no significant age-related factors. If pregnancy does not occur after 3–4 IUI cycles, IVF is often considered the next step.
A Clear Path Forward Exists. Let Us Find Yours.
Unexplained infertility is not the end of the road. It is an invitation to approach your fertility more strategically, with the right treatment at the right time, guided by someone who has helped thousands of couples in exactly your situation find their way through.
If you are in Lucknow or anywhere in Uttar Pradesh and would like a personalised consultation to map the right next step for you, I would like to meet you.
Personalised consultation
Book a personalised fertility consultation
Unexplained infertility, failed IUI cycles, or unsure whether to move to IVF. Map the right next step with Dr. Chauhan at Ganga Laxmi IVF, Gomti Nagar.
- Clinic
- 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow, 226010
- Hours
- Monday to Saturday, 9:00 AM to 8:00 PM
- Phone
- +91 72756 49692
- First consultation
- From Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
Unexplained infertility & IUI
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles
Male Infertility Treatment in Lucknow: Causes, Tests & Complete Guide
Male factors contribute to roughly half of all infertility cases. Dr. Kumudini Chauhan explains what causes male infertility, what a proper investigation looks like, and which treatments, from lifestyle changes to ICSI, are available at Ganga Laxmi IVF, Lucknow.

Laser Hatching and PGT After Failed IVF: Why Your Previous Cycles Failed and What to Do Next
Dr. Kumudini Chauhan explains why IVF fails, how Laser Assisted Hatching and PGT address those specific causes, and what a proper failed-IVF workup looks like at Ganga Laxmi IVF.

IVF After 40 in Lucknow: Advanced Age Fertility, PGT, and Realistic Hope
Fewer eggs, more chromosomal errors, harder decisions. Dr. Kumudini Chauhan explains what age actually does to your fertility, how PGT changes the odds, and what advanced age IVF looks like at Ganga Laxmi IVF, Lucknow.
PCOS and Pregnancy: Can You Conceive with PCOS?
Irregular cycles, no ovulation, conflicting advice. Dr. Kumudini Chauhan explains what PCOS actually does to your fertility, which treatments work at each stage, and what to expect at Ganga Laxmi IVF, Lucknow.