More women today are pursuing parenthood after 40 than at any point in the history of reproductive medicine. Some have spent their thirties managing health conditions that needed to be stabilised first. Some are in second marriages and building new families. Some simply could not make the timing work earlier and are here now, asking what is still possible.
I do not approach these consultations with a script. Every woman over 40 who comes to my clinic in Gomti Nagar, Lucknow, has a different set of test results, a different hormonal profile, and a different understanding of what she is willing to do. My job is to give her accurate information, not generic reassurance, and not unnecessary discouragement.
The honest picture: IVF is possible after 40, and for many women, it succeeds. But it requires a frank understanding of the biology, a carefully designed treatment plan, and in some cases, the willingness to consider options you may not have expected to need. Preimplantation Genetic Testing, or PGT, is one of the tools that has most meaningfully changed outcomes for older patients, and I will explain exactly why.
Quick Facts About IVF After 40
- IVF is possible after 40. Many women in their forties conceive successfully, either with their own eggs or with donor eggs.
- Egg quality is a greater challenge than egg quantity. After 40, the proportion of chromosomally abnormal embryos rises steeply — from roughly 40 to 55% at age 38 to 40, to 70 to 80% or more after 42.
- PGT-A (Preimplantation Genetic Testing) helps identify chromosomally normal embryos before transfer, reducing failed implantation and miscarriage risk, and improving the efficiency of each cycle.
- Miscarriage risk increases with maternal age — early pregnancy loss in women over 40 is approximately 40 to 50%, compared to 10 to 15% in women under 35. Most of this increase is caused by aneuploid embryos.
- Low ovarian reserve does not automatically rule out IVF. Fewer eggs means a smaller cohort, but it does not mean zero viable embryos. Natural cycle IVF and egg banking across cycles are options.
- Donor egg IVF remains an effective option for women whose own-egg cycles are not producing euploid embryos. Success rates with donor eggs are typically 50 to 60% per transfer, largely independent of the recipient's age.
- Under the ART (Regulation) Act, 2021, the legal maximum age for IVF in India is 50 years for women and 55 years for men.
How Does Age Affect Fertility? The Biology Explained
The decline in female fertility with age is not a myth, not an exaggeration, and not something that lifestyle changes can fully reverse. It is a biological fact rooted in the nature of the female reproductive system, and understanding it clearly is the foundation of any honest conversation about IVF after 40.
Women are born with all the eggs they will ever have, approximately one to two million at birth. By puberty, that number has fallen to around 300,000 to 500,000. By the mid-thirties, the rate of decline accelerates. By 40, the quantity of remaining eggs has reduced substantially, and more importantly, the quality of those eggs has also declined significantly.
Egg quality, in clinical terms, means chromosomal integrity. A healthy egg contains the correct number of chromosomes (23) that will combine with the 23 from the sperm to produce an embryo with the correct total of 46. As eggs age, errors in this chromosome segregation process become increasingly common. The resulting embryo may have too many or too few chromosomes, a state called aneuploidy. Aneuploid embryos either fail to implant, miscarry in early pregnancy, or in rare cases result in births with chromosomal conditions.
Under 35
Estimated % of Aneuploid Embryos
20 to 30%
35 to 37
Estimated % of Aneuploid Embryos
30 to 40%
38 to 40
Estimated % of Aneuploid Embryos
40 to 55%
41 to 42
Estimated % of Aneuploid Embryos
55 to 65%
Over 42
Estimated % of Aneuploid Embryos
70 to 80%+
| Age | Estimated % of Aneuploid Embryos |
|---|---|
| Under 35 | 20 to 30% |
| 35 to 37 | 30 to 40% |
| 38 to 40 | 40 to 55% |
| 41 to 42 | 55 to 65% |
| Over 42 | 70 to 80%+ |
Sources: CDC SART age-stratified data; ESHRE guidelines on advanced maternal age; Luma Fertility analysis of IVF cycles by age
This table explains why:
- Implantation rates decline with age even when embryos look normal on visual grading
- Miscarriage rates rise with age because aneuploid embryos that do implant often miscarry in the first trimester
- More eggs are needed to produce one viable embryo as age increases
- PGT becomes progressively more valuable as the proportion of abnormal embryos rises
This is about egg biology. It is not about overall health, fitness, diet, or effort. A fit and healthy 42-year-old has roughly the same egg quality picture as a sedentary 42-year-old. This is one of the most important things I tell patients, because many women arrive blaming themselves. There is nothing to blame.
Key clinical fact
After age 40, the majority of embryos produced in an IVF cycle may be chromosomally abnormal.
This is why transferring any morphologically acceptable embryo without genetic testing can result in repeated implantation failure or recurrent miscarriage, even in women who respond well to stimulation and produce multiple embryos.

IVF Success Rates After 40: What Research Shows
Understanding your realistic chances before starting treatment is something I consider a clinical obligation, not an option. The figures below are drawn from the most reliable available sources: the CDC's national ART surveillance data tracked through SART, and ESHRE's published analyses of age-stratified IVF outcomes.
40
Live Birth Rate (Own Eggs, per cycle)
15 to 20%
Clinical Context
Significant aneuploidy rate; PGT-A strongly recommended
41
Live Birth Rate (Own Eggs, per cycle)
12 to 18%
Clinical Context
Reserve and quality declining; PGT and ICSI standard protocol
42
Live Birth Rate (Own Eggs, per cycle)
10 to 15%
Clinical Context
Majority of embryos likely aneuploid; PGT essential
43
Live Birth Rate (Own Eggs, per cycle)
5 to 10%
Clinical Context
Very high aneuploidy rate; donor egg discussion appropriate
44 and above
Live Birth Rate (Own Eggs, per cycle)
Below 5%
Clinical Context
Own-egg IVF rarely viable; donor egg IVF primary recommendation
| Age | Live Birth Rate (Own Eggs, per cycle) | Clinical Context |
|---|---|---|
| 40 | 15 to 20% | Significant aneuploidy rate; PGT-A strongly recommended |
| 41 | 12 to 18% | Reserve and quality declining; PGT and ICSI standard protocol |
| 42 | 10 to 15% | Majority of embryos likely aneuploid; PGT essential |
| 43 | 5 to 10% | Very high aneuploidy rate; donor egg discussion appropriate |
| 44 and above | Below 5% | Own-egg IVF rarely viable; donor egg IVF primary recommendation |
Sources: CDC SART National ART Surveillance; ESHRE advanced maternal age guidance; ASRM Committee Opinion on Age and Fertility
Important: Success rates vary significantly based on ovarian reserve, embryo quality, laboratory standards, underlying fertility factors, and individual medical circumstances. These figures represent population-level data. After assessing your AMH, antral follicle count, prior cycle history, and complete hormonal profile, I give you an individual estimate, not a population average.
What PGT does to these numbers: When a euploid (chromosomally normal) embryo is transferred, implantation rates rise to approximately 60 to 70% regardless of the patient's age. The challenge in older patients is producing enough embryos to find at least one euploid one, not the transfer itself. This is the core clinical logic behind PGT after 40.
IVF for Advanced Age: What Changes After 40?
IVF treatment after 40 uses the same fundamental process as IVF at any other age: ovarian stimulation, egg retrieval, fertilisation in the lab, embryo culture, and embryo transfer. What changes is how that process must be designed, what expectations are realistic, and which additional tools are worth using.
Ovarian stimulation protocol
How It Changes After 40
Older ovaries often have lower reserve. Higher doses are not always better — they can produce fewer, poorer quality eggs if the ovary is forced
My Approach at Ganga Laxmi IVF
Individualised low-to-moderate stimulation based on AMH, antral follicle count, and body weight. The goal is optimal egg quality, not maximum egg numbers
ICSI alongside IVF
How It Changes After 40
With fewer eggs available per cycle, maximising fertilisation rate from every egg is critical
My Approach at Ganga Laxmi IVF
ICSI achieves fertilisation in approximately 70 to 85% of mature eggs. I recommend ICSI routinely for advanced age patients to avoid losing eggs at the fertilisation stage
Blastocyst culture (Day 5)
How It Changes After 40
Culturing to Day 5 allows only developmentally competent embryos to reach blastocyst stage. Weaker embryos arrest before Day 5
My Approach at Ganga Laxmi IVF
Where embryo numbers allow, I culture to blastocyst. It is far better to identify non-viable embryos in the lab than after a failed transfer
Fresh vs frozen transfer
How It Changes After 40
Optimal strategy depends on individual endometrial response, not a standard protocol
My Approach at Ganga Laxmi IVF
I assess the lining carefully before every transfer decision. Frozen transfer in a prepared cycle is preferred when lining quality after stimulation is suboptimal
PGT-A
How It Changes After 40
After 40, the proportion of aneuploid embryos is high enough that transferring without testing is a significant clinical risk
My Approach at Ganga Laxmi IVF
I discuss PGT with every patient over 40. It is not mandatory, but the clinical case is strong — particularly with prior miscarriage or failed transfers
Success rate counselling
How It Changes After 40
IVF success rates with own eggs decline significantly after 40
My Approach at Ganga Laxmi IVF
I have this conversation at the first consultation, not after failed cycles. Patients deserve honest numbers before they begin
| Parameter | How It Changes After 40 | My Approach at Ganga Laxmi IVF |
|---|---|---|
| Ovarian stimulation protocol | Older ovaries often have lower reserve. Higher doses are not always better — they can produce fewer, poorer quality eggs if the ovary is forced | Individualised low-to-moderate stimulation based on AMH, antral follicle count, and body weight. The goal is optimal egg quality, not maximum egg numbers |
| ICSI alongside IVF | With fewer eggs available per cycle, maximising fertilisation rate from every egg is critical | ICSI achieves fertilisation in approximately 70 to 85% of mature eggs. I recommend ICSI routinely for advanced age patients to avoid losing eggs at the fertilisation stage |
| Blastocyst culture (Day 5) | Culturing to Day 5 allows only developmentally competent embryos to reach blastocyst stage. Weaker embryos arrest before Day 5 | Where embryo numbers allow, I culture to blastocyst. It is far better to identify non-viable embryos in the lab than after a failed transfer |
| Fresh vs frozen transfer | Optimal strategy depends on individual endometrial response, not a standard protocol | I assess the lining carefully before every transfer decision. Frozen transfer in a prepared cycle is preferred when lining quality after stimulation is suboptimal |
| PGT-A | After 40, the proportion of aneuploid embryos is high enough that transferring without testing is a significant clinical risk | I discuss PGT with every patient over 40. It is not mandatory, but the clinical case is strong — particularly with prior miscarriage or failed transfers |
| Success rate counselling | IVF success rates with own eggs decline significantly after 40 | I have this conversation at the first consultation, not after failed cycles. Patients deserve honest numbers before they begin |
What Is PGT? Preimplantation Genetic Testing Explained
PGT, short for Preimplantation Genetic Testing, tests embryos for chromosomal abnormalities before transfer. Only chromosomally normal (euploid) embryos are selected. Embryos found to be aneuploid are not transferred.
The process: embryos are cultured to Day 5 blastocyst stage. A small biopsy is taken from the outer layer of cells, the trophectoderm, which will become the placenta. This biopsy of 5 to 8 cells does not sample the inner cell mass that becomes the baby itself. The cells are sent for chromosomal analysis. Results take 5 to 7 days, during which embryos are vitrified (frozen). Transfer takes place in a prepared cycle once results confirm chromosomal status.
PGT-A (Aneuploidy)
What It Tests
All 24 chromosomes for correct number
When Used
Advanced age (over 38), recurrent miscarriage, repeated IVF failure, reduced ovarian reserve
PGT-M (Monogenic)
What It Tests
Specific single-gene conditions (e.g. thalassemia, sickle cell, cystic fibrosis)
When Used
When either partner carries a known single-gene condition
PGT-SR (Structural Rearrangements)
What It Tests
Chromosomal translocations or inversions
When Used
When a parent carries a known chromosomal structural rearrangement
| Type | What It Tests | When Used |
|---|---|---|
| PGT-A (Aneuploidy) | All 24 chromosomes for correct number | Advanced age (over 38), recurrent miscarriage, repeated IVF failure, reduced ovarian reserve |
| PGT-M (Monogenic) | Specific single-gene conditions (e.g. thalassemia, sickle cell, cystic fibrosis) | When either partner carries a known single-gene condition |
| PGT-SR (Structural Rearrangements) | Chromosomal translocations or inversions | When a parent carries a known chromosomal structural rearrangement |
For advanced age patients, PGT-A is the relevant type. At Ganga Laxmi IVF in Lucknow, PGT is available for advanced age patients, those with recurrent IVF failure, and those with a history of recurrent miscarriage or recurrent pregnancy loss. Results are reviewed with me personally before any transfer decision is made.

Why PGT Matters Most After 40
The case for PGT in younger patients with good egg quality is genuinely debated in reproductive medicine, because in those patients the majority of embryos are normal and PGT adds less incremental value. In patients over 40, the calculation is entirely different.
When 60 to 80% of your embryos may be chromosomally abnormal, transferring without PGT means you are statistically more likely to transfer an aneuploid embryo than a normal one.
Without PGT after 40:
- Higher rate of failed implantation per transfer
- First trimester miscarriage rates of 40 to 50%, compared to 10 to 15% in women under 35
- Emotional and financial cost of multiple failed cycles without knowing whether any embryos were viable
- No information on remaining frozen embryo viability
With PGT after 40:
- Only chromosomally normal embryos transferred
- Per-transfer implantation rates rise to approximately 60 to 70% for euploid embryos, regardless of maternal age
- Miscarriage risk drops substantially for euploid transfers
- If no euploid embryos are found, this is critical information — it guides the next decision, rather than leading to another failed transfer
Why PGT does not guarantee pregnancy: PGT identifies chromosomal status. It does not assess every cause of implantation failure. Uterine factors (polyps, thin lining, endometritis, adhesions) can prevent implantation even of a chromosomally normal embryo. This is why uterine evaluation before transfer is mandatory in my protocol for every advanced age patient. PGT is a powerful tool — not a standalone solution.
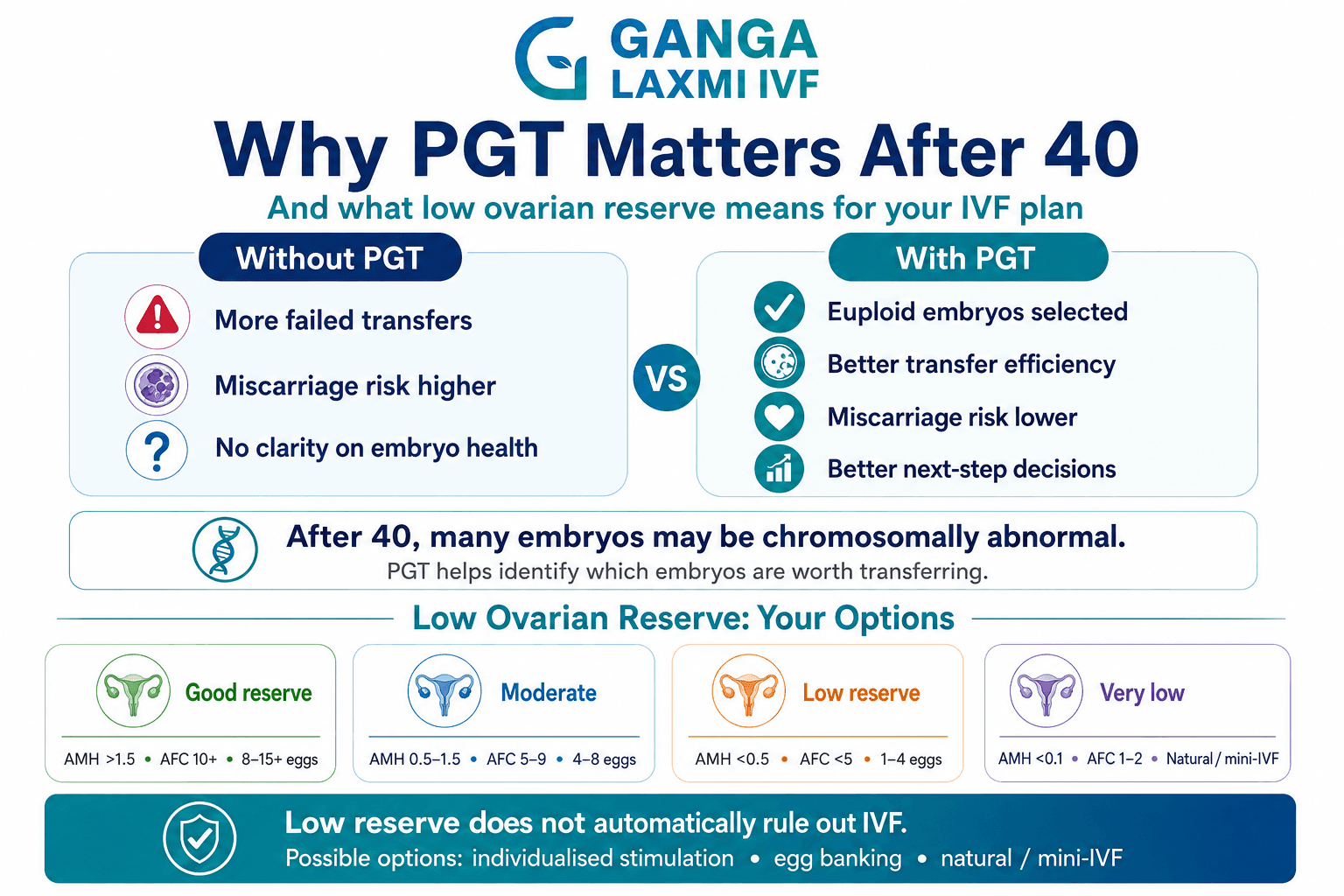
Low Ovarian Reserve and Advanced Age: Your Options
Low ovarian reserve is common in women over 40, though not universal. Some women in their early forties retain excellent reserve. Some women in their late thirties do not. Reserve is assessed primarily through AMH and antral follicle count (AFC). Low AMH treatment requires a different approach than standard IVF, and I design protocols accordingly.
Good reserve
AMH Level
Above 1.5 ng/mL
AFC
10 or more
Typical Response
8 to 15+ eggs; reasonable blastocyst and PGT cohort
Moderate reserve
AMH Level
0.5 to 1.5 ng/mL
AFC
5 to 9
Typical Response
4 to 8 eggs; smaller cohort but cycles remain viable
Low reserve (DOR)
AMH Level
Below 0.5 ng/mL
AFC
Fewer than 5
Typical Response
1 to 4 eggs; each cycle is precious; protocol design is critical
Very low reserve
AMH Level
Below 0.1 ng/mL
AFC
1 to 2
Typical Response
Natural cycle or mini-IVF may be preferred
| Reserve Status | AMH Level | AFC | Typical Response |
|---|---|---|---|
| Good reserve | Above 1.5 ng/mL | 10 or more | 8 to 15+ eggs; reasonable blastocyst and PGT cohort |
| Moderate reserve | 0.5 to 1.5 ng/mL | 5 to 9 | 4 to 8 eggs; smaller cohort but cycles remain viable |
| Low reserve (DOR) | Below 0.5 ng/mL | Fewer than 5 | 1 to 4 eggs; each cycle is precious; protocol design is critical |
| Very low reserve | Below 0.1 ng/mL | 1 to 2 | Natural cycle or mini-IVF may be preferred |
My approach for low reserve patients over 40:
- Individualised stimulation, not aggressive stimulation. High doses of gonadotrophins in a poor responder rarely produce significantly more eggs. They often produce the same number with higher cost and discomfort. I calibrate doses based on actual reserve markers.
- Egg banking across cycles. When reserve is genuinely low, a single cycle may yield one or two eggs. Accumulating embryos across two or three cycles before PGT gives a meaningful cohort and increases the probability of finding at least one euploid embryo.
- Natural cycle IVF. When stimulation produces only one or two follicles regardless of dose, a natural cycle IVF — retrieving the single egg the body produces naturally with minimal medication — is sometimes the right approach. Gentler, lower cost per cycle, and avoids forcing an ovary that has very little left.
Donor Egg IVF: An Honest Conversation
Many patients resist the idea of donor egg IVF when I first raise it. I understand why. It involves letting go of a significant expectation about what the journey would look like, and that deserves acknowledgement before any clinical discussion.
What I can tell you clinically: donor egg IVF offers the highest success rates of any fertility treatment available to women over 40, typically 50 to 60% per transfer. The eggs come from a young, screened donor whose egg quality is not affected by the recipient's age. The recipient's uterus carries the pregnancy. The genetic contribution is from the donor and the male partner. The pregnancy, the birth, the parenting, and the child are entirely yours in every meaningful sense.
Under the ART (Regulation) Act, 2021, donor eggs in India must come from an ever-married woman aged 23 to 35 with at least one living child of her own. Donors are screened for infectious diseases, genetic conditions, and chromosomal status. A donor may donate only once in her lifetime, and each donor's eggs may go to only one recipient couple.
Advanced Age IVF at Ganga Laxmi IVF, Lucknow
The clinical complexity of IVF after 40 demands a different level of attention than a standard IVF cycle, and I treat it that way.
AMH and Day 2-3 FSH, LH, Oestradiol
What It Tells Me
Quantifies ovarian reserve; FSH rising above 10 IU/L indicates declining reserve
Why It Matters After 40
Determines whether conventional stimulation is viable; guides dose selection and realistic expectations
Antral follicle count
What It Tells Me
Counts visible small follicles on the ovary
Why It Matters After 40
Most reliable real-time reserve indicator; directly predicts egg yield
Thyroid function (TSH)
What It Tells Me
Thyroid disorders are more common in women over 35
Why It Matters After 40
Untreated hypothyroidism is a common, correctable cause of implantation failure and recurrent miscarriage
Uterine evaluation
What It Tells Me
Assesses cavity for polyps, fibroids, adhesions, septum
Why It Matters After 40
Uterine factors must be resolved before any transfer, regardless of embryo quality
Fasting glucose and insulin
What It Tells Me
Insulin resistance affects endometrial receptivity
Why It Matters After 40
More common after 40; a modifiable factor I address before treatment
Vitamin D
What It Tells Me
Deficiency common in UP; impairs implantation
Why It Matters After 40
Simple to correct; meaningfully improves endometrial receptivity
Partner's semen analysis
What It Tells Me
Paternal age affects embryo quality; DNA fragmentation rises with male age
Why It Matters After 40
Advanced maternal age IVF produces precious few embryos — suboptimal sperm DNA can compromise their development
| Assessment | What It Tells Me | Why It Matters After 40 |
|---|---|---|
| AMH and Day 2-3 FSH, LH, Oestradiol | Quantifies ovarian reserve; FSH rising above 10 IU/L indicates declining reserve | Determines whether conventional stimulation is viable; guides dose selection and realistic expectations |
| Antral follicle count | Counts visible small follicles on the ovary | Most reliable real-time reserve indicator; directly predicts egg yield |
| Thyroid function (TSH) | Thyroid disorders are more common in women over 35 | Untreated hypothyroidism is a common, correctable cause of implantation failure and recurrent miscarriage |
| Uterine evaluation | Assesses cavity for polyps, fibroids, adhesions, septum | Uterine factors must be resolved before any transfer, regardless of embryo quality |
| Fasting glucose and insulin | Insulin resistance affects endometrial receptivity | More common after 40; a modifiable factor I address before treatment |
| Vitamin D | Deficiency common in UP; impairs implantation | Simple to correct; meaningfully improves endometrial receptivity |
| Partner's semen analysis | Paternal age affects embryo quality; DNA fragmentation rises with male age | Advanced maternal age IVF produces precious few embryos — suboptimal sperm DNA can compromise their development |
Why Women Across Lucknow and UP Choose Ganga Laxmi IVF
Advanced age IVF is not a standard fertility treatment. It requires specialist expertise in low ovarian reserve management, PGT-guided embryo selection, and recurrent IVF failure evaluation — a combination of skills that most general fertility clinics in the region do not offer under one roof.
What draws these patients is not advertising. It is word of mouth from couples who have been through failed cycles elsewhere and found, after coming to Ganga Laxmi IVF, that something important had been missed in their previous evaluation: an unchecked thyroid, an undertested uterine cavity, a stimulation protocol not calibrated to their actual reserve, or the absence of PGT in a patient who should have had it.
Why Trust Dr. Kumudini Chauhan for Advanced Age Fertility?
- Qualifications: MBBS, MS (Obstetrics and Gynaecology), DNB — the highest credentials
- Experience: 20+ years in clinical practice
- IVF volume: 8,000+ IVF cycles guided across career
- Continuity of care: Every patient sees Dr. Chauhan at every significant appointment.
Patient Stories
All names and identifying details changed with patient consent.
Sunita came to me after two failed IVF cycles at another clinic. Both cycles had produced embryos transferred without PGT, and neither resulted in implantation.
We corrected her thyroid, optimised her stimulation protocol, and conducted a PGT cycle. She produced five blastocysts. PGT found two euploid embryos. Her first frozen euploid transfer, with her thyroid optimised, resulted in a positive beta-hCG. She delivered a healthy boy at 42.
Sunita
41 years old, Lucknow
Reena had been through three IVF cycles with her own eggs before we met. Her AMH had fallen to 0.3 ng/mL. A fourth own-egg cycle produced one aneuploid blastocyst.
We discussed donor egg IVF and what it would mean for her. Her donor egg cycle was straightforward. A single blastocyst was transferred in a prepared cycle. She is now pregnant with twins.
Reena
43 years old, referred from Kanpur
Help centre
Frequently Asked Questions
These are the questions I hear every week from advanced age patients, including questions people hesitate to ask but absolutely should.
Under the Assisted Reproductive Technology (Regulation) Act, 2021, the legal maximum age for a woman to undergo IVF in India is 50 years. For men providing sperm, the limit is 55 years. These limits apply across all registered ART clinics in India including Ganga Laxmi IVF in Lucknow.
Yes. Using own eggs, the approximate live birth rate per IVF cycle is 15 to 20% at age 40, declining to below 5% at age 44 and above. PGT-A improves per-transfer outcomes by identifying chromosomally normal embryos before transfer. Donor egg IVF restores success rates to approximately 50 to 60% per transfer regardless of recipient age.
PGT-A (Preimplantation Genetic Testing for Aneuploidy) tests embryo cells for chromosomal normality before transfer. It is recommended for women aged 38 and above undergoing IVF, women with two or more miscarriages, women with two or more failed embryo transfers, and couples where a chromosomal structural rearrangement has been identified.
Yes. Low ovarian reserve requires an adapted protocol including individualised low-dose stimulation, natural cycle IVF where response is very low, and egg banking across cycles to build a sufficient embryo cohort before PGT. Fewer eggs does not mean zero viable embryos.
Natural conception at 42 is biologically possible but statistically uncommon due to high chromosomal error rates in eggs. If you have been trying for 6 months without success at age 42, a fertility evaluation is recommended rather than continuing to wait. Ovarian reserve declines continuously with age.
Whether IVF with own eggs is clinically worth trying at 43 depends entirely on individual reserve parameters. A 43-year-old with moderate AMH has a meaningfully different prognosis than one with very low AMH. PGT-A improves per-transfer outcomes. Donor egg IVF is a highly effective alternative when own-egg cycles are not producing euploid embryos.
After 40, AMH above 1.0 to 1.5 ng/mL is considered relatively well-preserved. AMH between 0.5 and 1.0 ng/mL indicates moderate reserve. Below 0.5 ng/mL is diminished ovarian reserve requiring an adapted protocol. Below 0.1 ng/mL is very low, where natural cycle IVF or donor egg IVF is the primary discussion. AMH is always interpreted alongside antral follicle count and the complete hormonal profile.
No. PGT-A screens embryos for chromosomal normality but does not test for all genetic conditions or guarantee implantation. Implantation also depends on uterine factors, endometrial receptivity, and other variables. PGT significantly reduces miscarriage risk and improves per-transfer success rates but is not a guarantee of a specific outcome.
IVF after 45 using own eggs is legally permitted in India up to age 50 under the ART Act, 2021. However, live birth rates with own eggs after 45 are below 5% per cycle. Donor egg IVF is the most clinically realistic path to pregnancy after 45, offering 50 to 60% success rates per transfer regardless of recipient age.
If PGT shows all embryos in a cohort are aneuploid, the options are: a further stimulation cycle to accumulate more embryos (if reserve allows), reassessment of the stimulation protocol, or transition to donor egg IVF. Finding no euploid embryo is not a failure — it is meaningful information that guides the next clinical decision.
Medical Guidelines and Research Referenced
The clinical information in this article is consistent with the following evidence base and regulatory framework:
- American Society for Reproductive Medicine (ASRM)
- European Society of Human Reproduction and Embryology (ESHRE)
- Centers for Disease Control and Prevention (CDC) / SART
- Indian ART (Regulation) Act, 2021
- POSEIDON Classification (2016)
You Have More Options Than the Statistics Suggest
If you are over 40 and want to understand what is genuinely possible for your specific situation, that conversation starts with a consultation and a few blood tests. Not with a statistic.
Advanced Age IVF Consultation
Book an Advanced Age IVF Consultation
Over 40 and want to understand your options clearly? Our fertility team will call you shortly.
- Clinic
- 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow, 226010
- Hours
- Monday to Saturday, 9:00 AM to 8:00 PM
- Phone
- +91 72756 49692
- First consultation
- From Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
Advanced Age IVF
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles
How to Increase AMH Levels: A Complete, Doctor Reviewed Guide
Can AMH levels really be increased? Learn what actually works, which foods and supplements may help, what science says, and when IVF is recommended. Doctor reviewed by fertility specialists at Ganga Laxmi IVF, Lucknow.

Blocked Fallopian Tube Treatment in Lucknow: Causes, HSG Test, IVF & Pregnancy Options
Blocked fallopian tubes are a leading cause of female infertility. Dr. Kumudini Chauhan explains causes, HSG testing and IVF options in Lucknow.

Azoospermia (Zero Sperm Count) Treatment in Lucknow
Diagnosed with zero sperm count? Dr. Kumudini Chauhan explains azoospermia causes and male infertility treatment with TESA, PESA, MicroTESE and ICSI in Lucknow.

Black Period Blood: Causes, Symptoms, Treatment and When to See a Doctor
Black period blood is usually harmless old blood, but it can signal PCOS, low estrogen or an infection. Know the causes, warning signs & when to consult a gynaecologist in Lucknow.