Quick Answer: Why Is My Period Blood Black?
Black period blood is almost always old blood - blood that has been sitting in the uterus long enough for oxygen to react with the iron in haemoglobin, turning it dark brown or black. This is called oxidation.
Black blood at the very beginning or end of your period is completely normal. It requires no treatment.
Black blood that lasts for most or all of your period, comes with pain or an unpleasant odour, is accompanied by irregular cycles, or appears after menopause - these warrant a gynaecologist's evaluation.
What Does Black Period Blood Actually Mean?
Normal menstrual blood is red - fresh blood that has moved quickly from the uterus through the cervix and out. The colour of period blood changes throughout the cycle based on one main variable: how long the blood spends inside the uterus before it exits.
Fresh blood that moves quickly stays red. Blood that moves slowly, or pools briefly, starts to oxidise. Oxidised blood is darker - ranging from burgundy to brown to black. The longer the delay, the darker the colour.
This is why you typically see the darkest blood at two points: right at the beginning, when flow is getting started and the first shed is moving slowly, and right at the end, when the last of the lining is emerging gradually.
The clinical question is not simply 'is my period blood black?' The better question is: is the black blood occurring at the expected time and in the expected amount, or is something else going on?
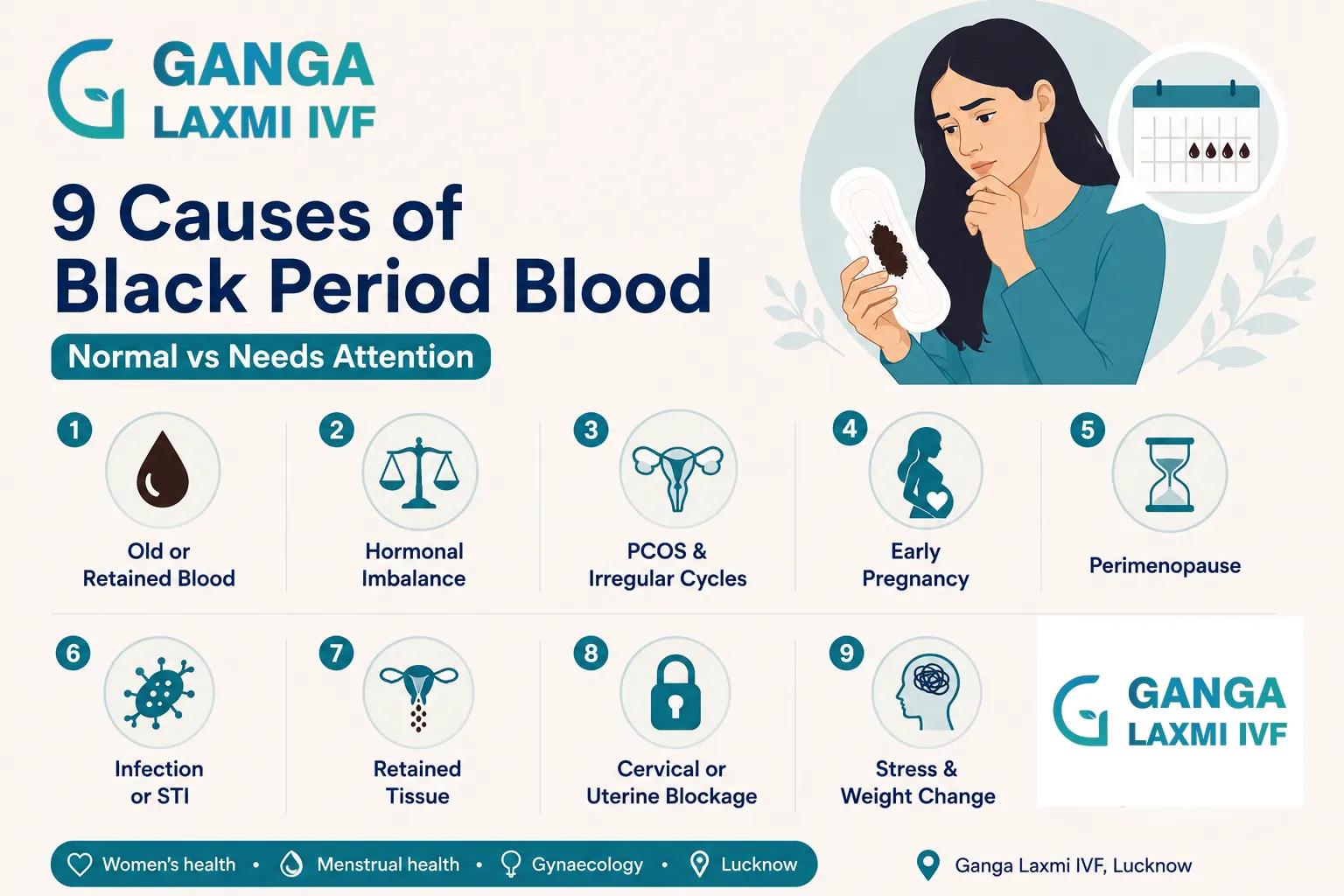
9 Common Causes of Black Period Blood
1. Old or Retained Blood at the Start or End of Your Cycle
This is by far the most common reason, and it is entirely normal. At the very start of your period, the uterine lining begins to shed but the flow rate is low. Blood moves slowly, stays in the uterus or cervix for longer, oxidises, and emerges dark brown or black. The same thing happens at the end of the period.
Signs this is the benign cause
- Appearing only on day one or the last day or two of your period
- Present in small amounts only - not sustained heavy flow
- No accompanying pain beyond typical period cramps
- Resolves as the flow increases or as the period ends completely
No investigation or treatment needed - this is your body's normal clearing process.
2. Hormonal Imbalance and Low Oestrogen
When oestrogen and progesterone are out of balance, the uterine lining may shed more slowly or unevenly, giving blood more time to oxidise. Low oestrogen is associated with a thinner lining that sheds slowly, producing darker, scantier blood. This can occur in:
If your periods have become consistently darker, lighter, and more infrequent, a hormonal assessment (FSH, LH, oestradiol, AMH) is worth discussing with your gynaecologist.
3. PCOS and Irregular Cycles
PCOS causes irregular or absent ovulation, meaning periods may be delayed by weeks or months. During that delay, old blood accumulates in the uterus. When the period eventually arrives, the first blood has been sitting there for an extended period and appears very dark or black as a result of oxidation.
Other PCOS symptoms that often accompany dark blood:
Read our PCOS and Pregnancy guide
4. Early Pregnancy and Implantation Bleeding
Implantation bleeding occurs when a fertilised egg embeds in the uterine lining (6 to 12 days after ovulation), producing light dark spotting often mistaken for a period.
Early miscarriage can also cause dark or black blood as early pregnancy tissue is passed, accompanied by cramping.
If your period is later than expected and the blood is unusually dark, a pregnancy test is a sensible first step.
5. Perimenopause and the Menopausal Transition
As oestrogen levels fluctuate and decline in perimenopause (typically 40s to 55), periods may arrive less frequently, with lighter or heavier flow and dark brown or black blood when cycles are long.
Important - post-menopausal bleeding
Any vaginal bleeding after menopause (12 consecutive months without a period) is NOT normal and must be evaluated promptly to rule out endometrial pathology.
6. Vaginal Infection, STI, or Pelvic Inflammatory Disease
Bacterial vaginosis (BV)
Fishy or musty odour, thin grey or dark discharge, mild itching or burning.
STIs (chlamydia, gonorrhoea)
Can cause cervicitis producing abnormal discharge and irregular dark bleeding.
Pelvic inflammatory disease (PID)
Pelvic pain, fever, offensive discharge, pain during intercourse. PID is a significant cause of infertility when untreated.
7. Retained Tissue After Miscarriage or Delivery
After a miscarriage or delivery, the body expels retained tissue, producing dark or black discharge for days to weeks as old blood clears gradually.
Seek urgent review if: heavy bright red bleeding not reducing after 24 hours, foul-smelling discharge, fever, or severe cramping - may indicate retained tissue requiring management.
8. Cervical or Uterine Blockage (Cervical Stenosis)
Cervical stenosis is a narrowing of the cervical canal through which menstrual blood exits. When blocked or narrowed, blood pools in the uterus, oxidises, and emerges very dark or black. Causes include prior cervical procedures (LLETZ, cone biopsy), congenital narrowing, or certain infections. Uterine fibroids and endometrial polyps can similarly obstruct blood flow.
Symptoms: very painful periods, decreased flow despite cramping, sensation of pressure.
9. Stress and Significant Weight Change
Significant physical or emotional stress, and rapid changes in body weight, can affect the hypothalamic-pituitary axis - the hormonal communication pathway between brain and ovaries. When disrupted, ovulation may be delayed or suppressed, cycles change, and periods become irregular or darker. Addressing the underlying stressor or weight stabilisation usually restores normal cycle patterns.
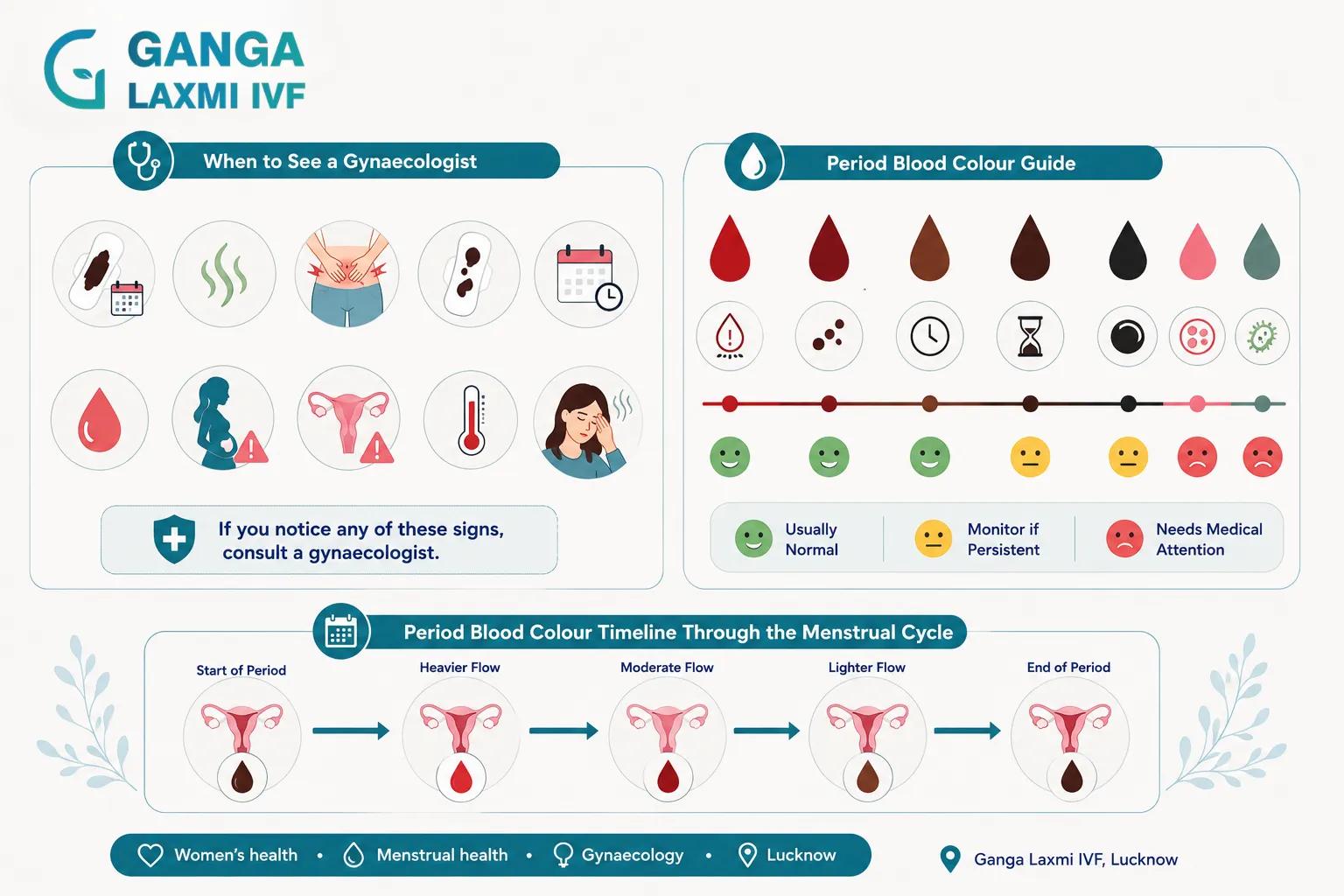
Is Black Period Blood Normal or a Red Flag?
It is usually normal when:
- Only on the first 1 to 2 days of your period, before the flow picks up
- Only on the last 1 to 2 days, as the flow tapers off
- Small amounts only - spotting rather than sustained flow
- No associated odour beyond the normal mild iron smell
- No unusual pain beyond typical period cramps
- Cycle length and frequency consistent with your normal pattern
- Occasional rather than consistently present every cycle
When to See a Gynaecologist
Black blood for most or all of your period (3+ days)
Why It Matters
Suggests old blood accumulation from slow flow or obstruction
Unpleasant or offensive odour
Why It Matters
Classic sign of infection - BV, STI, or PID
Severe pelvic pain beyond normal cramps
Why It Matters
May indicate endometriosis, PID, or cervical stenosis
Black blood with large clots
Why It Matters
Heavy old blood pooling - may indicate fibroids or endometrial pathology
Irregular cycles consistently
Why It Matters
Suggests hormonal imbalance, PCOS, or thyroid disorder
Black spotting between periods
Why It Matters
Intermenstrual bleeding requires evaluation to rule out structural causes
Black discharge in early pregnancy
Why It Matters
Must be assessed immediately - can indicate miscarriage or ectopic pregnancy
Any vaginal bleeding after menopause
Why It Matters
Always requires investigation regardless of colour
Fever, chills, or feeling systemically unwell
Why It Matters
Suggests active infection - seek urgent care
| Warning Sign | Why It Matters |
|---|---|
| Black blood for most or all of your period (3+ days) | Suggests old blood accumulation from slow flow or obstruction |
| Unpleasant or offensive odour | Classic sign of infection - BV, STI, or PID |
| Severe pelvic pain beyond normal cramps | May indicate endometriosis, PID, or cervical stenosis |
| Black blood with large clots | Heavy old blood pooling - may indicate fibroids or endometrial pathology |
| Irregular cycles consistently | Suggests hormonal imbalance, PCOS, or thyroid disorder |
| Black spotting between periods | Intermenstrual bleeding requires evaluation to rule out structural causes |
| Black discharge in early pregnancy | Must be assessed immediately - can indicate miscarriage or ectopic pregnancy |
| Any vaginal bleeding after menopause | Always requires investigation regardless of colour |
| Fever, chills, or feeling systemically unwell | Suggests active infection - seek urgent care |
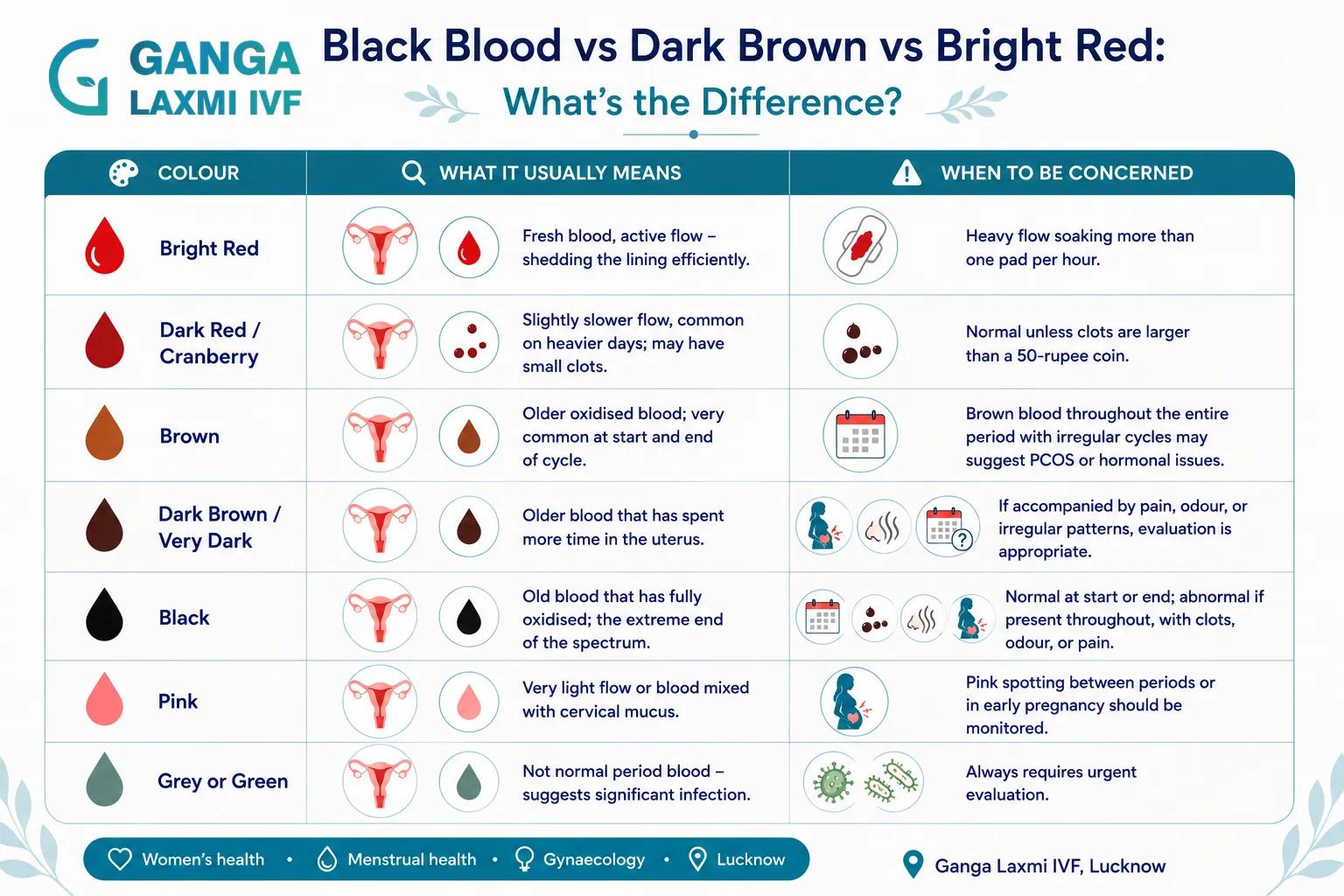
Black Blood vs Dark Brown vs Bright Red: What's the Difference?
Bright red
What It Usually Means
Fresh blood, active flow - shedding the lining efficiently
When to Be Concerned
Heavy flow soaking more than one pad per hour warrants evaluation
Dark red / cranberry
What It Usually Means
Slightly slower flow, common on heavier days; may have small clots
When to Be Concerned
Normal unless clots are larger than a 50-rupee coin
Brown
What It Usually Means
Older oxidised blood; very common at start and end of cycle
When to Be Concerned
Brown blood throughout the entire period with irregular cycles may suggest PCOS or hormonal issues
Dark brown / very dark
What It Usually Means
Older blood that has spent more time in the uterus
When to Be Concerned
If accompanied by pain, odour, or irregular patterns, evaluation is appropriate
Black
What It Usually Means
Old blood that has fully oxidised; the extreme end of the spectrum
When to Be Concerned
Normal at very start or end of a period; abnormal if present throughout, with clots, odour, or pain
Pink
What It Usually Means
Very light flow or blood mixed with cervical mucus
When to Be Concerned
Pink spotting between periods or in early pregnancy should be monitored
Grey or green
What It Usually Means
Not normal period blood - suggests significant infection
When to Be Concerned
Always requires urgent evaluation
| Colour | What It Usually Means | When to Be Concerned |
|---|---|---|
| Bright red | Fresh blood, active flow - shedding the lining efficiently | Heavy flow soaking more than one pad per hour warrants evaluation |
| Dark red / cranberry | Slightly slower flow, common on heavier days; may have small clots | Normal unless clots are larger than a 50-rupee coin |
| Brown | Older oxidised blood; very common at start and end of cycle | Brown blood throughout the entire period with irregular cycles may suggest PCOS or hormonal issues |
| Dark brown / very dark | Older blood that has spent more time in the uterus | If accompanied by pain, odour, or irregular patterns, evaluation is appropriate |
| Black | Old blood that has fully oxidised; the extreme end of the spectrum | Normal at very start or end of a period; abnormal if present throughout, with clots, odour, or pain |
| Pink | Very light flow or blood mixed with cervical mucus | Pink spotting between periods or in early pregnancy should be monitored |
| Grey or green | Not normal period blood - suggests significant infection | Always requires urgent evaluation |
How Ganga Laxmi IVF Diagnoses the Underlying Cause
At Ganga Laxmi IVF in Gomti Nagar, Lucknow, the investigation of abnormal period blood colour begins with a detailed history guided by what the history reveals.
The questions I ask in every consultation:
- When in the cycle does the dark blood appear - beginning, end, or throughout?
- How long has this been happening - recent change or long-standing pattern?
- Are your cycles regular? What is the length of your cycle?
- Is there any associated odour, pain, or discharge between periods?
- Any recent changes in weight, stress level, or exercise intensity?
- Any history of PCOS, thyroid disorder, or prior gynaecological procedures?
- Any possibility of pregnancy?
Pelvic / transvaginal ultrasound
What It Identifies
Uterine structure, fibroid or polyp detection, ovarian morphology (PCOS), endometrial thickness
Hormonal blood tests (FSH, LH, AMH, oestradiol, progesterone)
What It Identifies
Ovarian reserve, cycle phase assessment, PCOS hormonal pattern, perimenopause
Thyroid function (TSH, T3, T4)
What It Identifies
Hypothyroidism - a common and frequently missed cause of menstrual irregularity in India
Testosterone and prolactin
What It Identifies
Elevated in certain PCOS presentations; elevated prolactin can suppress ovulation
Vaginal swab / cervical smear
What It Identifies
Infection screening - bacterial vaginosis, STI, PID
Pregnancy test (urine or blood beta-hCG)
What It Identifies
Excludes pregnancy-related causes before proceeding with other investigations
Hysteroscopy
What It Identifies
Direct visualisation of uterine cavity - gold standard for polyps, adhesions, fibroids, cervical stenosis
Coagulation profile
What It Identifies
If heavy periods with significant clotting suggest a bleeding disorder
| Investigation | What It Identifies |
|---|---|
| Pelvic / transvaginal ultrasound | Uterine structure, fibroid or polyp detection, ovarian morphology (PCOS), endometrial thickness |
| Hormonal blood tests (FSH, LH, AMH, oestradiol, progesterone) | Ovarian reserve, cycle phase assessment, PCOS hormonal pattern, perimenopause |
| Thyroid function (TSH, T3, T4) | Hypothyroidism - a common and frequently missed cause of menstrual irregularity in India |
| Testosterone and prolactin | Elevated in certain PCOS presentations; elevated prolactin can suppress ovulation |
| Vaginal swab / cervical smear | Infection screening - bacterial vaginosis, STI, PID |
| Pregnancy test (urine or blood beta-hCG) | Excludes pregnancy-related causes before proceeding with other investigations |
| Hysteroscopy | Direct visualisation of uterine cavity - gold standard for polyps, adhesions, fibroids, cervical stenosis |
| Coagulation profile | If heavy periods with significant clotting suggest a bleeding disorder |
Treatment Options Depending on Cause
Normal oxidised blood at cycle edges
Treatment Approach
No treatment needed - reassurance and monitoring
PCOS
Treatment Approach
Hormonal regulation (OCP, progesterone, or metformin); ovulation induction if conception is the goal
Hormonal imbalance / low oestrogen
Treatment Approach
Hormone assessment and targeted supplementation; thyroid treatment if hypothyroidism identified
Vaginal infection / bacterial vaginosis
Treatment Approach
Appropriate antibiotics; partner treatment and STI screening if STI identified
Pelvic inflammatory disease (PID)
Treatment Approach
Broad-spectrum antibiotic combination; hospitalisation in severe cases
Uterine polyps
Treatment Approach
Hysteroscopic polypectomy - usually outpatient
Fibroids
Treatment Approach
Medical management (GnRH agonists, progesterone) or surgical intervention (myomectomy, hysteroscopic resection)
Cervical stenosis
Treatment Approach
Cervical dilation procedure; treatment of any underlying cause
Endometriosis
Treatment Approach
Medical suppression (hormonal therapy) or laparoscopic excision depending on severity
Perimenopause transition
Treatment Approach
Monitoring, lifestyle support; HRT if symptoms significantly affecting quality of life
Retained products after miscarriage
Treatment Approach
Medical management (misoprostol) or surgical evacuation (MVA or D&C)
Stress or weight-related changes
Treatment Approach
Addressing the underlying cause; nutritional support, stress management, lifestyle counselling
| Cause | Treatment Approach |
|---|---|
| Normal oxidised blood at cycle edges | No treatment needed - reassurance and monitoring |
| PCOS | Hormonal regulation (OCP, progesterone, or metformin); ovulation induction if conception is the goal |
| Hormonal imbalance / low oestrogen | Hormone assessment and targeted supplementation; thyroid treatment if hypothyroidism identified |
| Vaginal infection / bacterial vaginosis | Appropriate antibiotics; partner treatment and STI screening if STI identified |
| Pelvic inflammatory disease (PID) | Broad-spectrum antibiotic combination; hospitalisation in severe cases |
| Uterine polyps | Hysteroscopic polypectomy - usually outpatient |
| Fibroids | Medical management (GnRH agonists, progesterone) or surgical intervention (myomectomy, hysteroscopic resection) |
| Cervical stenosis | Cervical dilation procedure; treatment of any underlying cause |
| Endometriosis | Medical suppression (hormonal therapy) or laparoscopic excision depending on severity |
| Perimenopause transition | Monitoring, lifestyle support; HRT if symptoms significantly affecting quality of life |
| Retained products after miscarriage | Medical management (misoprostol) or surgical evacuation (MVA or D&C) |
| Stress or weight-related changes | Addressing the underlying cause; nutritional support, stress management, lifestyle counselling |
Frequently Asked Questions
Black blood on the first day of your period is almost always normal - old blood from the uterine lining of your previous cycle that has oxidised before your new period begins. As the flow increases, colour typically shifts to dark red or red. If blood remains black throughout multiple days, or is accompanied by pain, odour, or unusually light flow, see a gynaecologist.
Yes, in two specific situations. Implantation bleeding - when a fertilised egg embeds in the uterine lining around 6 to 12 days after ovulation - can produce a small amount of dark spotting. Early miscarriage can also cause dark or black blood. If your period arrives later than expected and the blood is unusually dark, a pregnancy test is the sensible first step.
Black or dark brown spotting 1 to 2 days before your period begins is generally normal - the uterine lining beginning to shed before the main flow starts. Spotting that begins more than 3 to 5 days before your expected period, or that occurs consistently every cycle, may indicate low progesterone in the luteal phase, which is treatable and worth investigating if you are trying to conceive.
Small clots smaller than a 50-rupee coin are normal. Larger clots, or consistently heavy clotting with dark blood, may indicate uterine fibroids, adenomyosis, a hormonal imbalance causing uneven shedding, or a bleeding disorder. If you are passing large clots or periods have become significantly heavier with dark, clotted blood, a pelvic ultrasound and hormonal assessment will help identify the cause.
Yes. PCOS causes irregular or absent ovulation, leading to delayed periods. When a period is delayed by weeks or months, old blood accumulates in the uterus and oxidises. When the period eventually arrives, the first blood appears very dark or black. If your cycles are consistently irregular and your period blood is frequently dark, PCOS investigation with ultrasound and hormonal blood tests is the appropriate starting point.
Both are oxidised blood - blood that has spent time in the uterus before exiting. Brown blood has oxidised moderately and is very common at the start and end of a normal period. Black blood has oxidised more completely, indicating a longer delay. The clinical significance depends on timing, duration, and associated symptoms rather than the exact shade. Both are normal at the edges of a cycle; both warrant evaluation if persistent throughout the period or accompanied by pain, odour, or irregular cycles.
Yes. Hypothyroidism (underactive thyroid) is a frequently overlooked cause of menstrual irregularity including dark or black period blood. Low thyroid function causes irregular, longer, heavier, or delayed periods - and delayed periods produce darker blood. TSH is a simple blood test that should be part of any initial investigation of menstrual irregularity, particularly in India where hypothyroidism is common.
Infection-related dark discharge is distinguishable by associated features: • An unpleasant, fishy, or foul odour - the most consistent sign of bacterial vaginosis and PID • Itching, burning, or irritation in the vaginal area • Pelvic or lower abdominal pain, particularly if constant rather than cyclical • Fever, feeling generally unwell • Discharge that is present outside of your period Normal period blood has a mild metallic iron odour but is not offensive. Any strong, unpleasant smell alongside dark discharge requires prompt evaluation.
When to Book a Consultation at Ganga Laxmi IVF, Lucknow
Book a consultation if any of the following apply:
- Your entire period consists of very dark or black blood
- Dark blood is accompanied by an odour, pain, or discharge between periods
- Cycles have become irregular or periods are arriving significantly less frequently
- Other signs of hormonal imbalance - weight change, hair changes, acne, excess facial hair
- You are trying to conceive and experiencing irregular cycles with dark blood
- You are in your 40s and noticing consistent changes in your period pattern
- You had a recent miscarriage or delivery and are unsure whether recovery is progressing normally
- Any bleeding after menopause - always requires assessment
Women come to Ganga Laxmi IVF in Gomti Nagar from across Lucknow - Indira Nagar, Aliganj, Hazratganj, Jankipuram, Faizabad Road - and from Kanpur, Barabanki, Sitapur, and Rae Bareli - for gynaecology consultations that go beyond a brief appointment.
Book a Gynaecology Consultation - Dr. Kumudini Chauhan, Lucknow
Ganga Laxmi IVF | 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow - 226010
Phone: +91 72756 49692 | Monday to Saturday, 9:00 AM to 8:00 PM
First Consultation: Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
IVF & fertility
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles

Kangaroo Mother Care (KMC): A Simple Yet Powerful Way to Save Newborn Lives
What is Kangaroo Mother Care? Learn how skin-to-skin contact saves premature babies, improves breastfeeding, and supports growth. A complete KMC guide.

IVF After a Failed Cycle: What to Do Next, and Why It Still Works
A failed IVF cycle does not mean the end. Dr. Kumudini Chauhan, Lucknow, explains what causes failure, what changes for the next cycle, and why many patients succeed after one setback.
Male Infertility Treatment in Lucknow: Causes, Tests & Complete Guide
Male factors contribute to roughly half of all infertility cases. Dr. Kumudini Chauhan explains what causes male infertility, what a proper investigation looks like, and which treatments, from lifestyle changes to ICSI, are available at Ganga Laxmi IVF, Lucknow.

Laser Hatching and PGT After Failed IVF: Why Your Previous Cycles Failed and What to Do Next
Dr. Kumudini Chauhan explains why IVF fails, how Laser Assisted Hatching and PGT address those specific causes, and what a proper failed-IVF workup looks like at Ganga Laxmi IVF.