If you have been through one or more IVF cycles without a successful pregnancy, you are not alone and you are not out of options. Recurrent implantation failure, defined clinically as the absence of pregnancy after transferring two or more good-quality embryos, affects approximately 10% of couples undergoing IVF. It is one of the most frustrating situations in reproductive medicine, because it involves going through the physical and emotional cost of a full treatment cycle only to have nothing take hold.
What I have learned after 20 years of treating patients with failed cycles is this: almost every patient who walks into my clinic in Gomti Nagar after failing elsewhere has something that was not properly evaluated. A missed thyroid abnormality. An embryo chromosomal error that PGT would have caught. An endometrial timing issue that ERA would have identified. A thickened zona pellucida in frozen embryos that Laser Hatching would have addressed.
Failed IVF is not evidence that your body cannot carry a pregnancy. In most cases, it is evidence that the previous approach was incomplete. The question after a failed cycle is never "should I give up?" The question is "what was missed?"
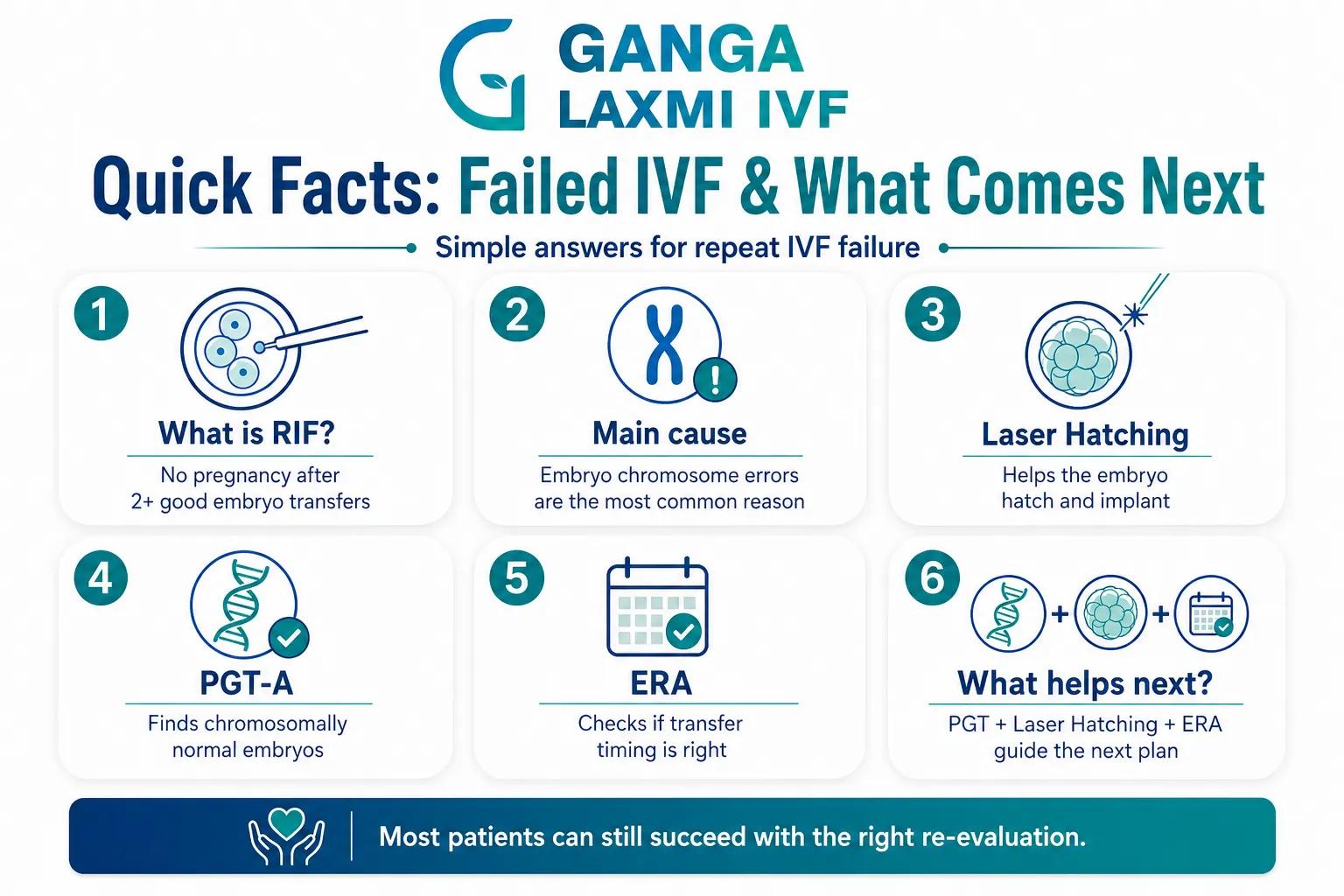
1. Quick Facts: Failed IVF and What Comes Next
- 1Recurrent implantation failure (RIF) is defined as failure to achieve pregnancy after transferring two or more good-quality embryos. It affects approximately 10% of IVF patients.
- 2The most common reason IVF fails is chromosomal abnormality in the embryo, which increases significantly with maternal age. This is the reason PGT exists.
- 3Laser Assisted Hatching helps embryos break through the outer shell (zona pellucida) to implant. It is particularly useful in frozen embryo transfers, advanced maternal age, and repeat implantation failure where the zona is thick or hardened.
- 4PGT-A (Preimplantation Genetic Testing for Aneuploidy) identifies chromosomally normal embryos before transfer. Patients with recurrent IVF failure who have not had PGT are very likely transferring aneuploid embryos without knowing it.
- 5ERA (Endometrial Receptivity Analysis) tests whether the endometrium is receptive at the time of transfer. A displaced window of implantation is found in a meaningful proportion of recurrent failure patients and is correctable.
- 6Combining PGT, Laser Hatching, and ERA as part of a structured recurrent failure workup addresses the three main causes of repeated implantation failure simultaneously.
- 7Most patients with recurrent IVF failure can achieve a successful pregnancy with a comprehensive re-evaluation and an appropriately redesigned treatment plan.
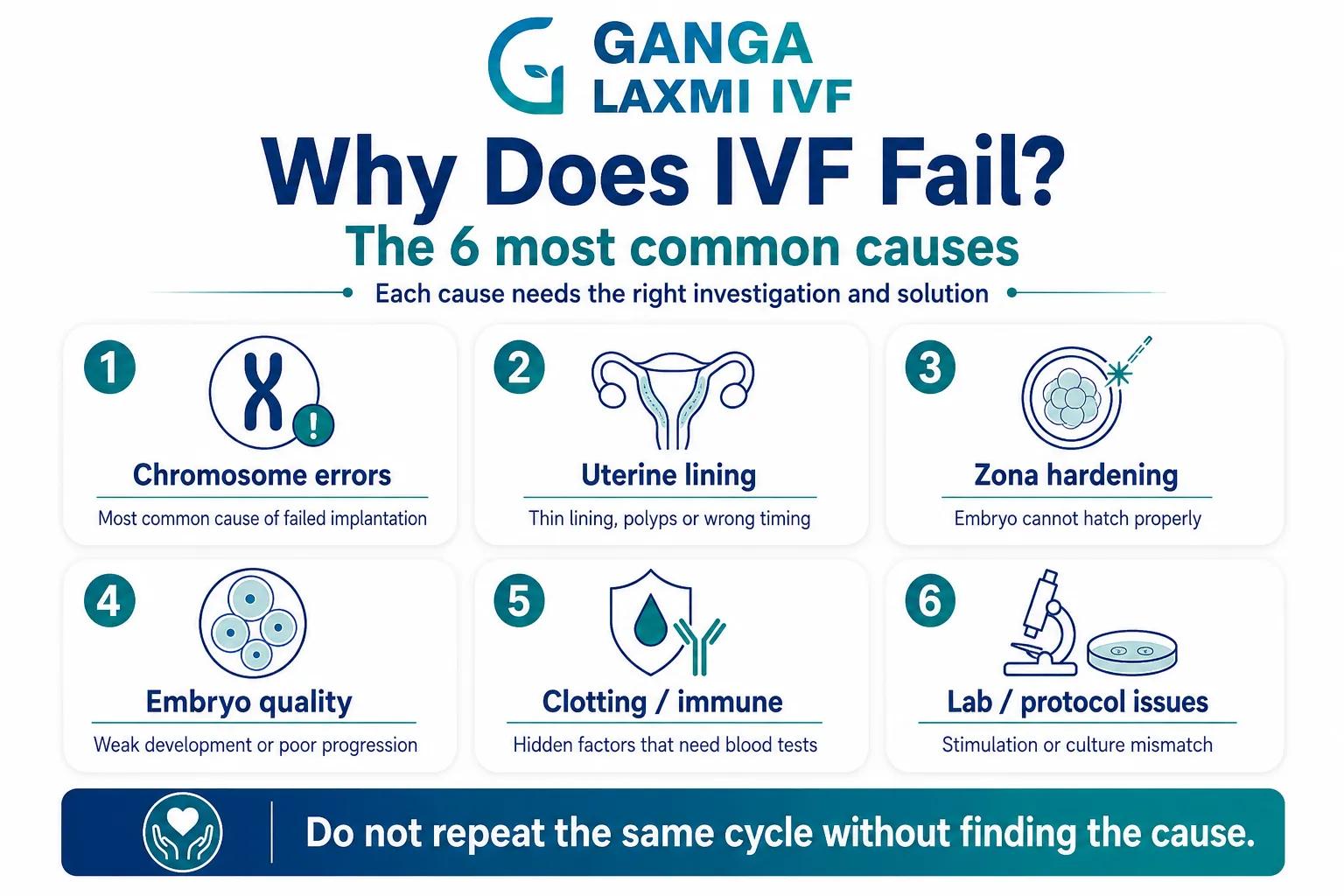
2. Why Does IVF Fail? The Most Common Causes
Before choosing any intervention for a failed IVF cycle, we need to understand what actually causes IVF to fail. This is not a rhetorical question. Each cause maps to a specific investigation and a specific solution, and treating the wrong cause is how patients end up going through another failed cycle.
The Main Causes of IVF Failure
Chromosomal abnormality in the embryo (aneuploidy)
Frequency
The single most common cause overall. Increases steeply with maternal age
What It Means Clinically
The embryo has too many or too few chromosomes. It fails to implant, or implants briefly and miscarries. Morphologically, these embryos can look completely normal under the microscope
Endometrial (uterine lining) factors
Frequency
Second most common category
What It Means Clinically
Thin lining, polyps, fibroids distorting the cavity, adhesions, endometritis (uterine infection), or a displaced window of implantation where the embryo is transferred at the wrong point in the receptivity cycle
Zona pellucida hardening
Frequency
More common in frozen embryo transfers, advanced maternal age, and high FSH patients
What It Means Clinically
The outer shell of the embryo becomes too thick or hardened to allow the embryo to hatch out and contact the uterine lining. The embryo may be chromosomally normal but physically unable to implant
Embryo quality issues
Frequency
Common in older patients, poor responders, and patients with sperm DNA fragmentation
What It Means Clinically
Poor cytoplasmic quality, fragmentation, or arrested development before or after transfer. Not always caused by chromosomal problems — sperm DNA integrity and culture conditions contribute
Thrombophilia and immunological factors
Frequency
Identified in a subset of recurrent failure patients
What It Means Clinically
Blood clotting disorders or immune responses that interfere with early implantation. Requires specific blood testing to diagnose
Suboptimal laboratory or stimulation conditions
Frequency
Less common but real
What It Means Clinically
Protocol mismatch, suboptimal stimulation for the patient's age and reserve, culture media quality, or ovarian hyperstimulation affecting endometrial receptivity in a fresh cycle
| Cause | Frequency | What It Means Clinically |
|---|---|---|
| Chromosomal abnormality in the embryo (aneuploidy) | The single most common cause overall. Increases steeply with maternal age | The embryo has too many or too few chromosomes. It fails to implant, or implants briefly and miscarries. Morphologically, these embryos can look completely normal under the microscope |
| Endometrial (uterine lining) factors | Second most common category | Thin lining, polyps, fibroids distorting the cavity, adhesions, endometritis (uterine infection), or a displaced window of implantation where the embryo is transferred at the wrong point in the receptivity cycle |
| Zona pellucida hardening | More common in frozen embryo transfers, advanced maternal age, and high FSH patients | The outer shell of the embryo becomes too thick or hardened to allow the embryo to hatch out and contact the uterine lining. The embryo may be chromosomally normal but physically unable to implant |
| Embryo quality issues | Common in older patients, poor responders, and patients with sperm DNA fragmentation | Poor cytoplasmic quality, fragmentation, or arrested development before or after transfer. Not always caused by chromosomal problems — sperm DNA integrity and culture conditions contribute |
| Thrombophilia and immunological factors | Identified in a subset of recurrent failure patients | Blood clotting disorders or immune responses that interfere with early implantation. Requires specific blood testing to diagnose |
| Suboptimal laboratory or stimulation conditions | Less common but real | Protocol mismatch, suboptimal stimulation for the patient's age and reserve, culture media quality, or ovarian hyperstimulation affecting endometrial receptivity in a fresh cycle |
The clinical principle I apply to every patient with failed IVF:
Before repeating the same cycle, I need to understand which of these causes was operative. A repeat cycle without a diagnosis is not a treatment plan. It is an expensive guess.
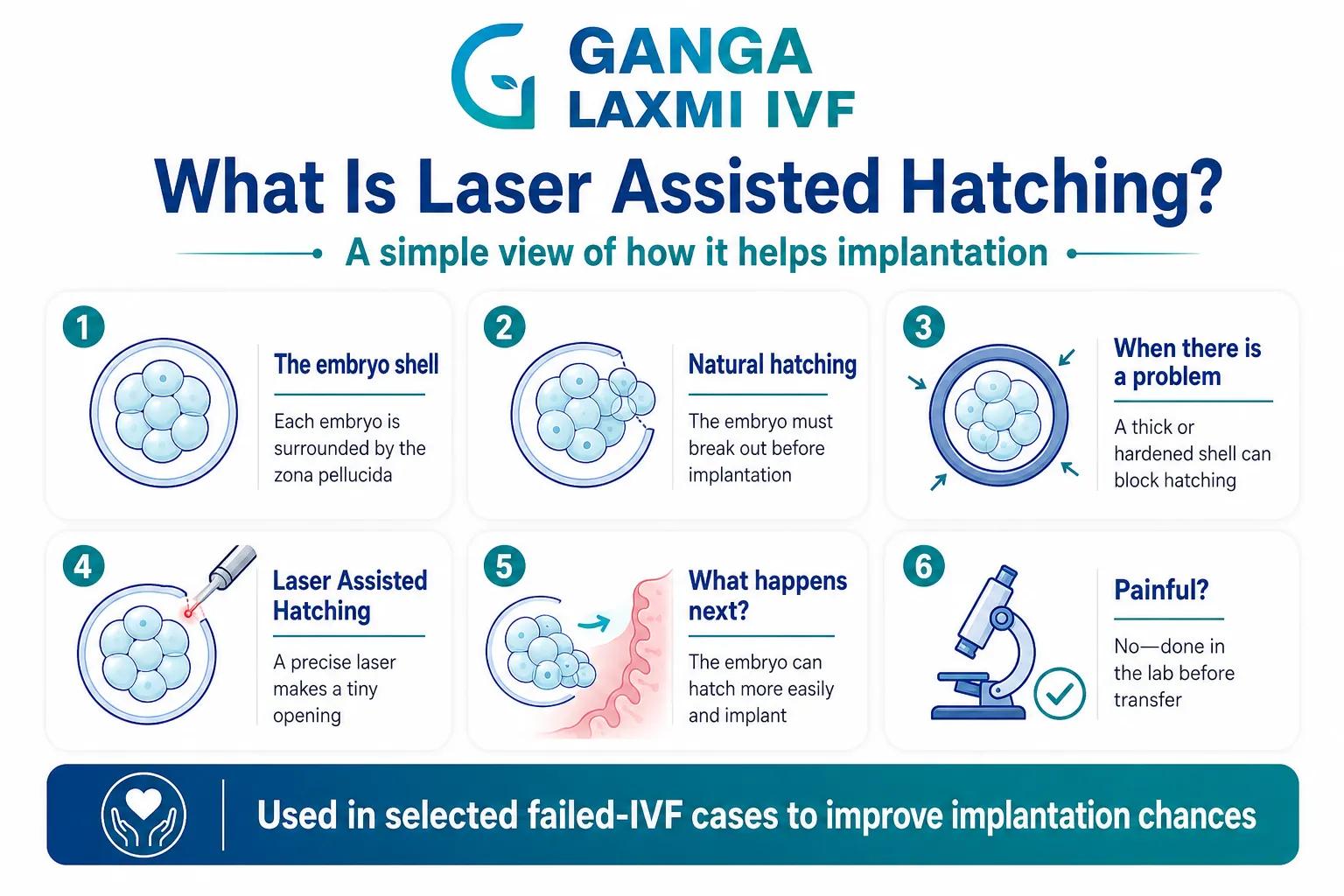
3. What Is Laser Assisted Hatching?
To understand why Laser Assisted Hatching matters in failed IVF, you need to understand what the embryo has to do before it can implant.
Every embryo is surrounded by a protective outer shell called the zona pellucida — a glycoprotein layer that forms around the egg at fertilisation and remains around the embryo through the early stages of development. For implantation to occur, the embryo must break through this shell, a process called hatching, and make direct contact with the endometrial lining. Only then can it embed and begin the process of implantation.
In most cases this happens naturally. But in several clinical situations, the zona pellucida becomes too thick, too hard, or too resistant for the embryo to hatch through on its own:
- Vitrification (freezing and thawing) can alter the zona's mechanical properties, making it harder than in a fresh cycle
- Advanced maternal age is associated with a naturally thicker zona pellucida
- Elevated FSH levels have been linked to zona hardening
- Prolonged in vitro culture can affect zona properties
- Previous failed implantation with morphologically good embryos, where the zona may be the unexplained barrier
Laser Assisted Hatching uses a highly precise infrared laser beam to create a small, controlled opening in the zona pellucida before the embryo is transferred. The embryologist applies the laser for a fraction of a second, creating an opening of approximately 20 to 40 micrometres — large enough to allow the embryo to hatch more readily, but small enough to leave the embryo intact and undamaged.
The laser is applied to the trophectoderm region of the blastocyst, away from the inner cell mass. At Ganga Laxmi IVF, Laser Assisted Hatching is performed by our trained embryology team using calibrated laser equipment, not improvised chemical or mechanical methods. Precision matters here — both under- and over-application produce suboptimal results.
Is Laser Hatching painful for the patient?
No. Laser Assisted Hatching is performed in the embryology laboratory, entirely outside the body. It is done on the embryo before transfer, under the microscope. The patient feels nothing at the hatching stage. The embryo transfer itself is a simple, minimally uncomfortable procedure — similar to a pap smear.
4. When Is Laser Hatching Recommended After Failed IVF?
Laser Assisted Hatching is not recommended for every IVF cycle. It is a targeted tool for specific clinical situations. After a failed cycle, these are the scenarios where I recommend it:
Frozen Embryo Transfer (FET) cycles
Why Laser Hatching Helps
Vitrification alters zona pellucida properties; hatching assistance is routinely beneficial
Evidence Basis
Cochrane Review and multiple RCTs show improved implantation rates in FET cycles with assisted hatching
Advanced maternal age (over 37)
Why Laser Hatching Helps
Natural zona thickening with age; embryos may have sufficient quality but fail to hatch
Evidence Basis
ASRM and ESHRE acknowledge assisted hatching as a reasonable intervention in this group
Elevated baseline FSH (above 10 IU/L)
Why Laser Hatching Helps
Associated with zona hardening even in younger patients
Evidence Basis
Observational evidence supports benefit in poor prognosis patients with elevated FSH
Recurrent implantation failure with morphologically good embryos
Why Laser Hatching Helps
When embryos have looked normal but failed to implant in multiple cycles, zona resistance is a plausible mechanical cause
Evidence Basis
Supported by ESHRE good practice recommendations on RIF (2023)
Thick zona pellucida noted by the embryologist
Why Laser Hatching Helps
Direct observation of zona thickness above normal range during embryo grading
Evidence Basis
Clinical indication; embryologist-led decision at biopsy or grading stage
Cleavage-stage (Day 3) transfers with slow development
Why Laser Hatching Helps
Slower embryos may benefit from hatching assistance to keep pace with uterine synchrony
Evidence Basis
Used selectively at the embryologist's judgement
| Clinical Situation | Why Laser Hatching Helps | Evidence Basis |
|---|---|---|
| Frozen Embryo Transfer (FET) cycles | Vitrification alters zona pellucida properties; hatching assistance is routinely beneficial | Cochrane Review and multiple RCTs show improved implantation rates in FET cycles with assisted hatching |
| Advanced maternal age (over 37) | Natural zona thickening with age; embryos may have sufficient quality but fail to hatch | ASRM and ESHRE acknowledge assisted hatching as a reasonable intervention in this group |
| Elevated baseline FSH (above 10 IU/L) | Associated with zona hardening even in younger patients | Observational evidence supports benefit in poor prognosis patients with elevated FSH |
| Recurrent implantation failure with morphologically good embryos | When embryos have looked normal but failed to implant in multiple cycles, zona resistance is a plausible mechanical cause | Supported by ESHRE good practice recommendations on RIF (2023) |
| Thick zona pellucida noted by the embryologist | Direct observation of zona thickness above normal range during embryo grading | Clinical indication; embryologist-led decision at biopsy or grading stage |
| Cleavage-stage (Day 3) transfers with slow development | Slower embryos may benefit from hatching assistance to keep pace with uterine synchrony | Used selectively at the embryologist's judgement |
Who is Laser Hatching not recommended for:
- Routine IVF cycles in patients under 35 with good reserve and no prior failure
- Patients transferring fresh, high-quality blastocysts with normal zona properties
- Patients where the likely cause of failure is chromosomal (PGT is the appropriate intervention, not Laser Hatching)
This distinction matters because I regularly see patients who have had Laser Hatching recommended as a generic "add-on" without any analysis of whether their failure was zona-related or chromosomal. Laser Hatching does not correct chromosomal errors. PGT does not assist hatching. They address entirely different mechanisms, and using the right tool for the right problem is what drives better outcomes.
5. What Is PGT and How Does It Address IVF Failure?
PGT (Preimplantation Genetic Testing) tests embryos for chromosomal abnormalities before transfer. I have covered PGT in detail in a separate article on IVF after 40, so here I want to focus specifically on its role in recurrent IVF failure.
Why is PGT so important after failed cycles?
Because chromosomal abnormality (aneuploidy) is the single most common reason embryos fail to implant or miscarry — and aneuploid embryos are indistinguishable from normal embryos on visual grading alone. An embryo that receives a top score from the embryologist on Day 5 — expanding blastocyst, clear inner cell mass, excellent trophectoderm — has approximately a 30 to 50% chance of being chromosomally abnormal depending on the patient's age. In a patient over 40, that figure rises to 60 to 80%.
This means that patients who have had two, three, or four "good embryos transferred" without pregnancy are almost certainly among those who have been transferring aneuploid embryos. They have not had implantation failure in the true sense. They have had chromosomally abnormal embryos failing to develop past the point of biochemical detection.
What PGT changes for recurrent failure patients:
Aneuploid and euploid embryos transferred interchangeably
With PGT Going Forward
Only chromosomally confirmed normal embryos transferred
Failed transfers attributed to "unexplained implantation failure"
With PGT Going Forward
Failed transfers correctly attributed to aneuploidy; fewer unnecessary investigations
Per-transfer implantation rate limited by proportion of aneuploid embryos
With PGT Going Forward
Per-transfer implantation rate rises to 60 to 70% for confirmed euploid embryos regardless of maternal age
Recurrent first-trimester loss due to aneuploid implantation
With PGT Going Forward
Miscarriage rate for euploid transfers approximately 8 to 13%, versus 25 to 50% without PGT in patients over 38
No information on embryo quality beyond morphology
With PGT Going Forward
Complete chromosomal status of each embryo — informs both current transfer and future cycle planning
| Without PGT in Previous Cycles | With PGT Going Forward |
|---|---|
| Aneuploid and euploid embryos transferred interchangeably | Only chromosomally confirmed normal embryos transferred |
| Failed transfers attributed to "unexplained implantation failure" | Failed transfers correctly attributed to aneuploidy; fewer unnecessary investigations |
| Per-transfer implantation rate limited by proportion of aneuploid embryos | Per-transfer implantation rate rises to 60 to 70% for confirmed euploid embryos regardless of maternal age |
| Recurrent first-trimester loss due to aneuploid implantation | Miscarriage rate for euploid transfers approximately 8 to 13%, versus 25 to 50% without PGT in patients over 38 |
| No information on embryo quality beyond morphology | Complete chromosomal status of each embryo — informs both current transfer and future cycle planning |
In a study of recurrent implantation failure patients using ERA combined with PGT-A, patients who opted for PGT-A had implantation rates of 88 to 95% and clinical pregnancy rates of 100% in both receptive and non-receptive ERA groups, compared to 34 to 37% clinical pregnancy rates in non-PGT-A patients. While this is a single-centre retrospective study and should be interpreted with appropriate caution, it illustrates what can be achieved when chromosomal selection and endometrial timing are addressed simultaneously.
PGT-A vs PGT-M: which applies in failed IVF?
For most recurrent failure patients, PGT-A is the relevant test — it screens all 24 chromosome pairs for correct copy number and is the standard tool for failed IVF without a known single-gene disorder. PGT-M (for monogenic conditions like thalassemia or cystic fibrosis) is used when a specific inherited condition needs to be screened for, and requires knowing what to look for before the cycle begins. The two tests address completely different problems and are not interchangeable.
At Ganga Laxmi IVF in Lucknow, PGT-A is available for recurrent failure patients. The biopsy is performed by our embryology team at blastocyst stage, and results are reviewed with me personally before any transfer decision is made.
6. Combining PGT and Laser Hatching: A Protocol for Repeat Failures
For patients who have had two or more failed IVF cycles, the most comprehensive and effective approach combines both interventions within a structured protocol. The logic is straightforward:
- PGT addresses the embryo side: it confirms which embryos are chromosomally viable before transfer, eliminating the most common cause of failed implantation.
- Laser Hatching addresses the mechanical side: it ensures that a chromosomally confirmed normal embryo is not prevented from implanting by a physical barrier — a zona that is too thick or hardened to allow the embryo to emerge and contact the lining.
These two causes can coexist. A patient may have been transferring aneuploid embryos (problem one) in a frozen cycle where the zona was also hardened (problem two). Correcting only one of these without the other leaves a significant probability of failure.
How the Combined Protocol Works at Ganga Laxmi IVF
Stimulation and retrieval
What Happens
Individualised protocol based on AMH, AFC, age. ICSI used routinely to maximise fertilisation of every egg
Blastocyst culture
What Happens
Embryos cultured to Day 5 or 6. Only embryos that develop to blastocyst stage are biopsied
PGT-A biopsy
What Happens
Trophectoderm cells biopsied and sent for chromosomal analysis. All embryos vitrified
Results review
What Happens
PGT results reviewed with patient. Transfer plan made based on euploid embryo availability
Frozen embryo transfer preparation
What Happens
Endometrial preparation in a separate cycle. ERA considered if prior failed transfers even with euploid embryos
Laser Hatching
What Happens
Applied to the euploid blastocyst on the morning of transfer, 2 to 3 hours before the procedure
Transfer
What Happens
Single euploid blastocyst transferred under ultrasound guidance
Beta-hCG
What Happens
Pregnancy test at day 14 post-transfer
| Stage | What Happens |
|---|---|
| Stimulation and retrieval | Individualised protocol based on AMH, AFC, age. ICSI used routinely to maximise fertilisation of every egg |
| Blastocyst culture | Embryos cultured to Day 5 or 6. Only embryos that develop to blastocyst stage are biopsied |
| PGT-A biopsy | Trophectoderm cells biopsied and sent for chromosomal analysis. All embryos vitrified |
| Results review | PGT results reviewed with patient. Transfer plan made based on euploid embryo availability |
| Frozen embryo transfer preparation | Endometrial preparation in a separate cycle. ERA considered if prior failed transfers even with euploid embryos |
| Laser Hatching | Applied to the euploid blastocyst on the morning of transfer, 2 to 3 hours before the procedure |
| Transfer | Single euploid blastocyst transferred under ultrasound guidance |
| Beta-hCG | Pregnancy test at day 14 post-transfer |
This is not a one-size-fits-all protocol. Some recurrent failure patients need only PGT. Some need only ERA. Some need only Laser Hatching on frozen transfers. The protocol is built around the individual investigation findings — which is why the workup comes before the protocol decision.
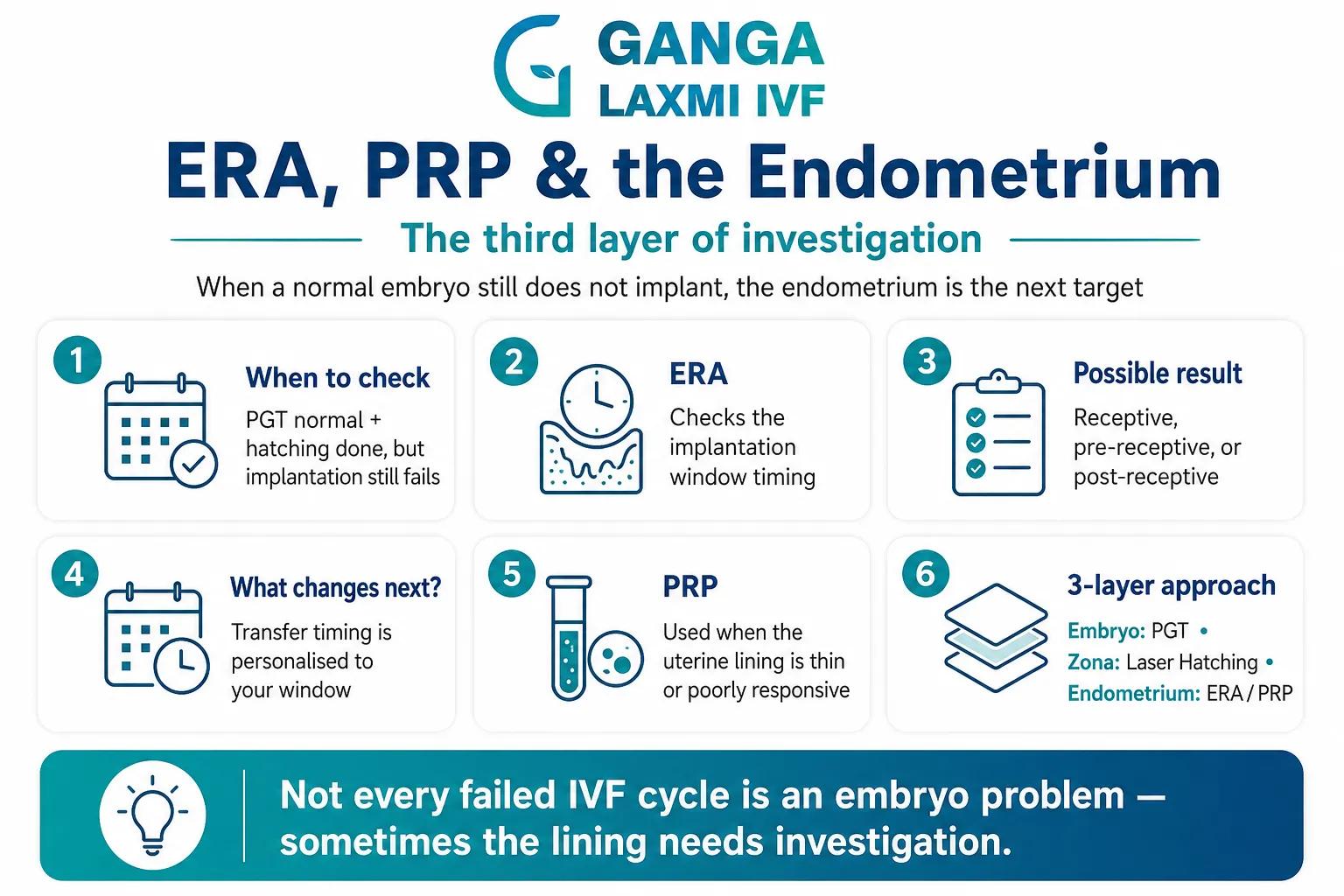
7. Endometrial Receptivity, ERA, and PRP: The Third Layer of Investigation
If PGT has confirmed a chromosomally normal embryo and Laser Hatching has ensured the embryo can hatch — but implantation still does not occur — the endometrium is the next investigation target.
ERA (Endometrial Receptivity Analysis)
The endometrium has a "window of implantation" — a specific window of time, typically 3 to 4 days after progesterone supplementation begins in a frozen cycle, during which it is maximally receptive to an embryo. In most patients, this window occurs at the standard timing. In approximately 25 to 30% of patients with recurrent implantation failure, the window is displaced, meaning the endometrium is not yet receptive, or is past peak receptivity, at the time of standard transfer.
ERA is a biopsy of the endometrial lining taken during a mock transfer cycle. The sample is analysed using gene expression profiling to determine whether the endometrium is receptive, pre-receptive, or post-receptive at the moment of biopsy. If a displacement is identified, the subsequent embryo transfer is timed to match the patient's personal window — a Personalised Embryo Transfer (pET).
In a study of recurrent implantation failure patients who underwent ERA, those in the non-receptive group who had their embryo transfer adjusted to their receptivity window achieved clinical pregnancy rates of 73.5% and implantation rates of 78.6%. This is a meaningful improvement in a population that had previously experienced repeated failure.
The honest caveat about ERA: The evidence is not uniformly positive. A JAMA-published trial in unselected IVF patients (not specifically RIF) showed no benefit from ERA-guided transfer. The current ESHRE position is that ERA is not recommended for routine IVF, but is reasonable in recurrent implantation failure patients, particularly where previous failures have occurred despite euploid transfers. This is exactly the population I offer it to.
Endometrial PRP (Platelet-Rich Plasma)
For patients with a thin or poorly responsive endometrium — where the lining does not reach the 7 to 8 mm thickness needed for optimal implantation despite standard hormonal preparation — Endometrial PRP is an option I use at Ganga Laxmi IVF.
PRP is prepared from the patient's own blood by centrifugation to concentrate growth factors. When infused into the uterine cavity, it promotes endometrial growth and blood vessel formation. Published studies in thin lining patients show improvements in endometrial thickness and in clinical pregnancy rates, though the evidence remains observational rather than from large randomised trials. For patients who have had multiple cycles cancelled due to thin lining, or whose prior transfers involved a suboptimal lining, it is a reasonable intervention with no significant side effects.
8. The Full Recurrent IVF Failure Workup at Ganga Laxmi IVF, Lucknow
When a patient comes to me after failed IVF cycles — whether two or five — I do not immediately recommend another cycle. I start with a complete re-evaluation.
What I Assess After Failed IVF
Review of all prior cycle records
What It Identifies
Protocol, doses, stimulation response, embryo grades, transfer timing, and any PGT results
Why It Matters for Repeat Failure
Most commonly missed: whether any euploid embryos were ever confirmed; whether stimulation was appropriate for the patient's reserve
AMH, FSH, AFC repeat
What It Identifies
Current ovarian reserve status
Why It Matters for Repeat Failure
Reserve can change between cycles; the protocol that was appropriate 18 months ago may not be appropriate now
TSH (thyroid)
What It Identifies
Thyroid dysfunction
Why It Matters for Repeat Failure
One of the most commonly missed causes of recurrent implantation failure; I have found hypothyroidism in multiple patients who failed elsewhere without any thyroid testing
Thrombophilia screen
What It Identifies
Factor V Leiden, prothrombin gene mutation, antiphospholipid antibodies, MTHFR
Why It Matters for Repeat Failure
Blood clotting disorders cause implantation failure and are treatable with low-dose aspirin and/or heparin
Immunological testing
What It Identifies
NK cell activity, antinuclear antibodies
Why It Matters for Repeat Failure
In selected patients with unexplained RIF where embryo and uterine causes have been excluded
Hysteroscopy
What It Identifies
Polyps, adhesions, septum, submucosal fibroids, endometritis
Why It Matters for Repeat Failure
Critical before any further transfer; uterine cavity abnormalities are found in 25 to 40% of RIF patients when properly evaluated
Endometrial biopsy for CD138
What It Identifies
Chronic endometritis
Why It Matters for Repeat Failure
Plasma cell inflammation in the uterine lining is found in approximately 30% of RIF patients and is treatable with antibiotics
Partner's semen analysis + DNA fragmentation
What It Identifies
Sperm DNA integrity
Why It Matters for Repeat Failure
Sperm DNA fragmentation impairs embryo development and blastocyst quality — a cause of poor embryo cohorts that is frequently overlooked in female-focused evaluations
ERA (if previous euploid transfer failed)
What It Identifies
Window of implantation displacement
Why It Matters for Repeat Failure
Offered when a chromosomally confirmed normal embryo has failed to implant — the most targeted indication for ERA
Vitamin D, fasting insulin, glucose
What It Identifies
Modifiable systemic factors
Why It Matters for Repeat Failure
Deficiencies and insulin resistance are common in UP and are modifiable before any further treatment
| Investigation | What It Identifies | Why It Matters for Repeat Failure |
|---|---|---|
| Review of all prior cycle records | Protocol, doses, stimulation response, embryo grades, transfer timing, and any PGT results | Most commonly missed: whether any euploid embryos were ever confirmed; whether stimulation was appropriate for the patient's reserve |
| AMH, FSH, AFC repeat | Current ovarian reserve status | Reserve can change between cycles; the protocol that was appropriate 18 months ago may not be appropriate now |
| TSH (thyroid) | Thyroid dysfunction | One of the most commonly missed causes of recurrent implantation failure; I have found hypothyroidism in multiple patients who failed elsewhere without any thyroid testing |
| Thrombophilia screen | Factor V Leiden, prothrombin gene mutation, antiphospholipid antibodies, MTHFR | Blood clotting disorders cause implantation failure and are treatable with low-dose aspirin and/or heparin |
| Immunological testing | NK cell activity, antinuclear antibodies | In selected patients with unexplained RIF where embryo and uterine causes have been excluded |
| Hysteroscopy | Polyps, adhesions, septum, submucosal fibroids, endometritis | Critical before any further transfer; uterine cavity abnormalities are found in 25 to 40% of RIF patients when properly evaluated |
| Endometrial biopsy for CD138 | Chronic endometritis | Plasma cell inflammation in the uterine lining is found in approximately 30% of RIF patients and is treatable with antibiotics |
| Partner's semen analysis + DNA fragmentation | Sperm DNA integrity | Sperm DNA fragmentation impairs embryo development and blastocyst quality — a cause of poor embryo cohorts that is frequently overlooked in female-focused evaluations |
| ERA (if previous euploid transfer failed) | Window of implantation displacement | Offered when a chromosomally confirmed normal embryo has failed to implant — the most targeted indication for ERA |
| Vitamin D, fasting insulin, glucose | Modifiable systemic factors | Deficiencies and insulin resistance are common in UP and are modifiable before any further treatment |
A complete workup takes one to two cycles and a few blood tests. Another failed cycle without this workup takes three months, significant financial cost, and an enormous emotional toll — and still leaves the question unanswered.
After this evaluation, I have a clear picture of what was operative in the failed cycles and a specific rationale for every element of the new protocol. That conversation happens with you directly before any new cycle begins.
9. Patient Story: Three Failures, One Right Diagnosis
Name and identifying details changed with patient consent.
Anjali had three failed IVF cycles at two different clinics before coming to me. All three cycles had produced Day 5 blastocysts that were graded as good or excellent. All three had been frozen transfers. None had resulted in implantation. She had been told there was no explanation.
When I reviewed her records, the first thing I noticed was that no PGT had ever been done. All six embryos transferred across three cycles had been selected on morphology alone. At age 37, the proportion of chromosomally abnormal embryos is approximately 40 to 55%. It was entirely possible that all six transferred embryos had been aneuploid.
Her thyroid had been checked once, early in the first clinic's workup. Her TSH at that point was 3.8 mIU/L. Not flagged as abnormal using a standard reference range, but above the 2.5 threshold I recommend for fertility patients. Over the following 18 months across three cycles, it had never been rechecked. When I tested it, it was 5.1 mIU/L.
Her hysteroscopy was normal. Her thrombophilia screen was negative. Her CD138 endometrial biopsy was negative for chronic endometritis.
We corrected her thyroid to below 2.5, designed a new stimulation cycle, and performed PGT on all blastocysts. She produced four blastocysts. Two were euploid. Her first frozen euploid transfer was also her first transfer with Laser Hatching applied, given three prior failed frozen transfers.
Her beta-hCG at day 14 was positive. She is currently in her second trimester.
Three cycles of failure, two causes that had never been investigated: chromosomal status and thyroid function. One cycle with the right workup, and the outcome was entirely different.
Anjali
37 years old, Indira Nagar, Lucknow
10. Frequently Asked Questions
A proper recurrent failure workup should begin after two failed cycles with good-quality embryos. Waiting longer delays identification of a treatable cause and reduces ovarian reserve further. Causes like chronic endometritis, hypothyroidism, thrombophilia, and displaced window of implantation do not resolve without treatment and will cause every subsequent cycle to fail.
No. Laser Hatching addresses one specific cause: zona pellucida hardening or thickening. It does not correct chromosomal abnormalities, uterine lining problems, or immunological causes. It is most effective in frozen embryo transfers, advanced maternal age, and recurrent failure where zona resistance is a contributing factor.
PGT-A screens all 24 chromosomes for correct copy number and is the test used for recurrent IVF failure and advanced maternal age. PGT-M tests for a specific known single-gene disorder and requires knowing what to look for before the cycle. Most recurrent failure patients need PGT-A, not PGT-M.
No. Laser Assisted Hatching is performed in the embryology laboratory on the embryo before transfer. The patient is not involved in or affected by this procedure. The embryo transfer itself takes approximately 10 minutes and is described by most patients as similar to a cervical smear.
ERA (Endometrial Receptivity Analysis) tests whether your endometrial window of implantation is displaced. It is recommended specifically when a chromosomally confirmed normal embryo has failed to implant, or when recurrent failure has occurred despite a normal uterine cavity and normal systemic investigations. It is not recommended for routine IVF.
Laser Assisted Hatching is typically priced between Rs. 10,000 and Rs. 20,000 per cycle. PGT-A costs are quoted per embryo or per cycle cohort and include the lab biopsy and specialist genetics analysis. A failed-IVF workup consultation starts at Rs. 400. Costs are discussed transparently before any cycle begins.
You Deserve a Diagnosis, Not Another Cycle
IVF failure is not a verdict. It is an incomplete investigation.
Every patient who comes to me after failed cycles at other clinics gets the same starting point: a full review of what was done, what was not done, and what the most likely operative cause of failure was. In the majority of cases, at least one actionable finding emerges. A thyroid that was never rechecked. Embryos that were never chromosomally tested. A uterine cavity that was never properly evaluated. A thrombophilia that was never screened for.
Laser Hatching and PGT are powerful tools. They work best when they are applied to the right patient for the right reason, as part of a complete clinical evaluation, not as reflexive add-ons to an unchanged protocol.
If you have been through IVF without success, I would like to review your case. The conversation starts at ₹400 and a few hours of your time. The outcome may be entirely different from what you have experienced before.
Recurrent IVF failure consultation
Book Your Consultation
Most patients who come to me after failed cycles elsewhere have at least one missed diagnosis. Let's find it.
- Clinic
- 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow, 226010
- Hours
- Monday to Saturday, 9:00 AM to 8:00 PM
- Phone
- +91 72756 49692
- First consultation
- From Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
IVF & fertility
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles
How to Increase AMH Levels: A Complete, Doctor Reviewed Guide
Can AMH levels really be increased? Learn what actually works, which foods and supplements may help, what science says, and when IVF is recommended. Doctor reviewed by fertility specialists at Ganga Laxmi IVF, Lucknow.

Blocked Fallopian Tube Treatment in Lucknow: Causes, HSG Test, IVF & Pregnancy Options
Blocked fallopian tubes are a leading cause of female infertility. Dr. Kumudini Chauhan explains causes, HSG testing and IVF options in Lucknow.

Azoospermia (Zero Sperm Count) Treatment in Lucknow
Diagnosed with zero sperm count? Dr. Kumudini Chauhan explains azoospermia causes and male infertility treatment with TESA, PESA, MicroTESE and ICSI in Lucknow.

Black Period Blood: Causes, Symptoms, Treatment and When to See a Doctor
Black period blood is usually harmless old blood, but it can signal PCOS, low estrogen or an infection. Know the causes, warning signs & when to consult a gynaecologist in Lucknow.