I see PCOS every single day in my clinic in Gomti Nagar. It is the most common hormonal condition in women of reproductive age in India, affecting approximately 1 in 5 Indian women, and it is also, without question, the most commonly misunderstood cause of infertility I encounter.
Some patients arrive after years of being told their cycles will “regulate on their own.” Some have been given oral contraceptives without any fertility discussion. A few come to me having spent months blaming themselves for their weight, their stress, their diet, as if the diagnosis were somehow a personal failure.
I want to be direct with you about two things: PCOS is a medical condition, not a lifestyle consequence. And PCOS does not mean permanent infertility. It means your path to pregnancy may need medical support, and that support is now very effective.
This article explains exactly what PCOS does to your fertility, which treatments work at each stage, and what honest success looks like for women with PCOS who want to conceive.
What Is PCOS and How Does It Affect Fertility?
Polycystic Ovary Syndrome is a hormonal imbalance affecting how the ovaries function. Despite the name, “polycystic” does not mean the ovaries are filled with cysts in the traditional sense. What it describes is the appearance of many small, undeveloped follicles, each containing an immature egg, that accumulate because ovulation is not completing normally.
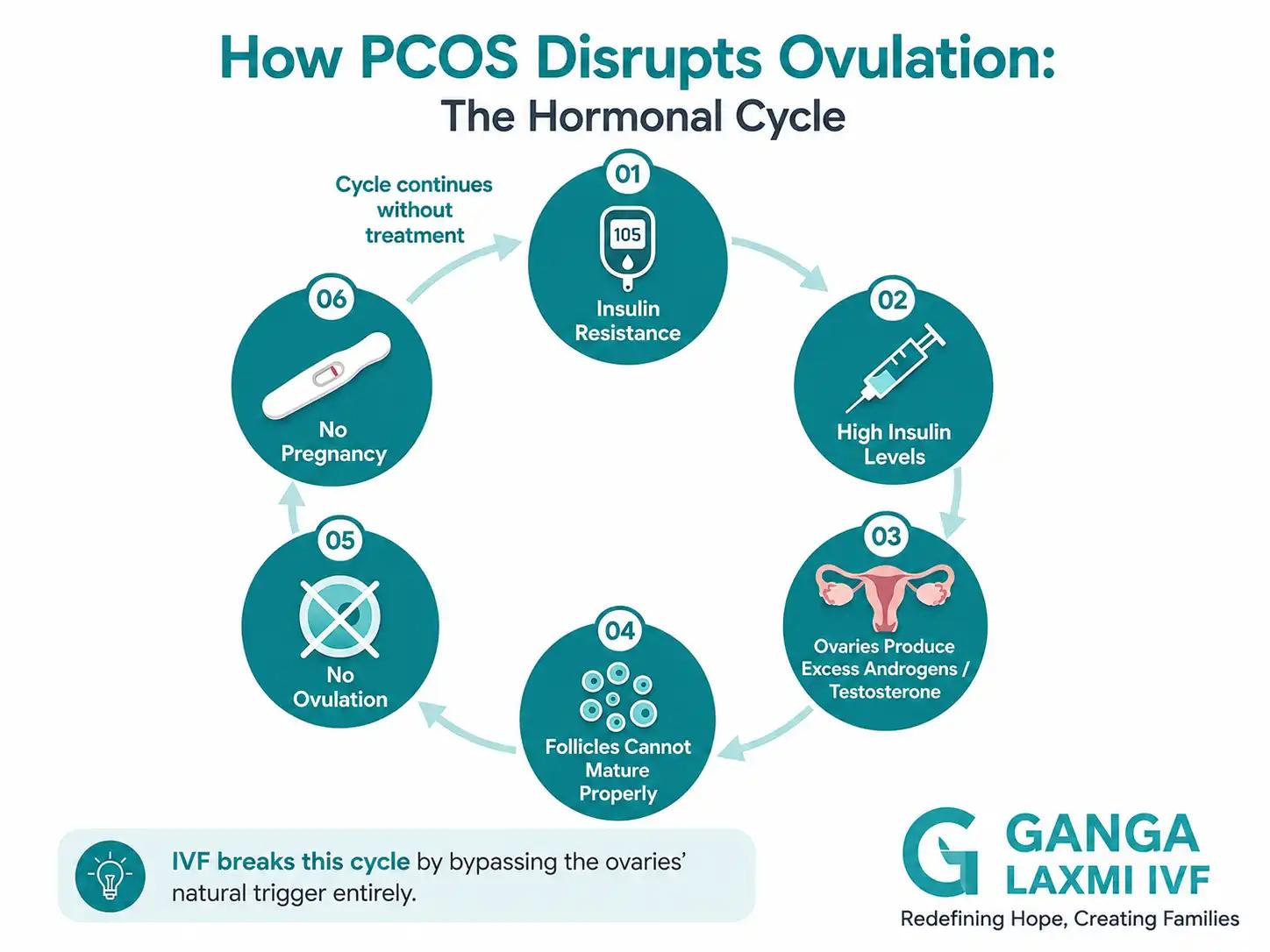
The Core Hormonal Disruption
In a healthy menstrual cycle, hormonal signals from the brain trigger the development and release of a single mature egg each month. In PCOS, this process is disrupted at multiple levels:
LH (Luteinising Hormone)
What Happens in PCOS
Elevated, often disproportionately high relative to FSH
Effect on Fertility
Disrupts follicle maturation; egg is not released
Androgens (Testosterone)
What Happens in PCOS
Ovaries produce excess testosterone
Effect on Fertility
Interferes with follicle development and egg quality
Insulin
What Happens in PCOS
Many PCOS patients have insulin resistance
Effect on Fertility
Excess insulin stimulates the ovaries to produce more androgens, creating a compounding cycle
AMH (Anti-Müllerian Hormone)
What Happens in PCOS
Significantly elevated in PCOS
Effect on Fertility
Reflects large number of small follicles; confirms PCOS on investigation
Progesterone
What Happens in PCOS
Low because ovulation is not completing
Effect on Fertility
No corpus luteum forms; uterine lining is not adequately prepared for implantation
| Hormone | What Happens in PCOS | Effect on Fertility |
|---|---|---|
| LH (Luteinising Hormone) | Elevated, often disproportionately high relative to FSH | Disrupts follicle maturation; egg is not released |
| Androgens (Testosterone) | Ovaries produce excess testosterone | Interferes with follicle development and egg quality |
| Insulin | Many PCOS patients have insulin resistance | Excess insulin stimulates the ovaries to produce more androgens, creating a compounding cycle |
| AMH (Anti-Müllerian Hormone) | Significantly elevated in PCOS | Reflects large number of small follicles; confirms PCOS on investigation |
| Progesterone | Low because ovulation is not completing | No corpus luteum forms; uterine lining is not adequately prepared for implantation |
The practical result of this hormonal disruption is anovulation, meaning the ovaries are not releasing a mature egg regularly. Without ovulation, natural pregnancy cannot occur.
Key clinical fact
PCOS is the leading cause of anovulatory infertility worldwide, accounting for approximately 70–80% of all anovulatory infertility cases.
It is also the most treatable. The ovaries in PCOS are not damaged. They are dysregulated. With the right treatment, ovulation can often be restored.
Common Symptoms That Bring Patients to My Clinic
- Irregular, infrequent, or absent periods (cycles longer than 35 days, or fewer than 8 periods per year)
- Difficulty conceiving after 6–12 months of trying
- Excess facial or body hair (hirsutism)
- Acne, particularly on the jawline and chin
- Thinning scalp hair
- Weight gain, especially around the abdomen
- Darkened skin patches around the neck, armpits, or groin (acanthosis nigricans, a sign of insulin resistance)
- Ultrasound showing multiple small follicles arranged around the periphery of the ovary (“string of pearls” appearance)
Not every patient with PCOS has all of these symptoms. Some women have completely regular periods and still have PCOS, which is exactly why a blood test and ultrasound are essential for accurate diagnosis.
Can Women with PCOS Get Pregnant Naturally?
The honest answer is: yes, many can, but it takes longer, and it does not happen for everyone without support.
Women with PCOS who have at least some spontaneous ovulation, even if irregular, do conceive naturally. The key variables are age, the severity of hormonal imbalance, and whether there are additional fertility factors in either partner.
When Natural Conception Is Worth Trying
If you are under 35, have been trying for fewer than 12 months, have a partner with normal semen parameters, and have no additional diagnoses (blocked tubes, endometriosis, uterine abnormalities), a structured lifestyle approach while monitoring ovulation is a reasonable starting point.
Lifestyle changes are not a minor footnote in PCOS management. They are first-line treatment, because in women with PCOS and insulin resistance, even a 5–10% reduction in body weight can restore spontaneous ovulation. The mechanism is direct: lower insulin levels reduce androgen production by the ovaries, which allows follicles to mature normally.
That said, I am careful about how I communicate this with patients. Weight loss is not always straightforward, and telling a woman to “just lose weight” without a structured plan is not a clinical recommendation. It is unhelpful and often demoralising.
When to Stop Waiting and Seek Evaluation
Please do not wait indefinitely. I see patients who have spent three or four years hoping their cycles will “sort themselves out.” Ovarian reserve declines with age regardless of PCOS, and earlier treatment gives you more options with better outcomes.
Seek a fertility evaluation if:
- You are under 35 and have been trying for 12 months without success
- You are 35 or older and have been trying for 6 months without success
- Your cycles are consistently longer than 35 days, absent, or completely unpredictable
- You have a confirmed PCOS diagnosis and want to conceive within the next 1–2 years
- You have any coexisting condition: thyroid disorder, diabetes, prior miscarriage, or endometriosis symptoms
Treatment Options for PCOS and Fertility, Step by Step
At Ganga Laxmi IVF, I always start with the least invasive option that is appropriate for your specific clinical picture. I do not recommend IVF to every PCOS patient who walks in the door. Many women with PCOS conceive with ovulation induction and IUI. What matters is matching the treatment to the diagnosis, not escalating unnecessarily, and not staying on ineffective treatment for too long.

Step 1: Lifestyle Optimisation and Insulin Sensitisation
Weight loss (5–10% body weight)
What It Does
Reduces insulin and androgen levels; restores spontaneous ovulation in many patients
Evidence
Well-established first-line recommendation in PCOS international guidelines
Low glycaemic index (low GI) diet
What It Does
Reduces insulin spikes; improves hormonal balance
Evidence
Consistent benefit seen in clinical studies
Regular aerobic + strength exercise
What It Does
Improves insulin sensitivity independently of weight loss
Evidence
Effective even without significant weight change
Metformin
What It Does
Insulin-sensitising medication; improves ovulation rate and reduces androgen levels
Evidence
Particularly beneficial in PCOS patients with insulin resistance or elevated fasting glucose
Inositol (myo-inositol + D-chiro-inositol)
What It Does
Improves insulin signalling; shown to improve ovulation and egg quality in PCOS
Evidence
Growing evidence base; I discuss this with selected patients
| Intervention | What It Does | Evidence |
|---|---|---|
| Weight loss (5–10% body weight) | Reduces insulin and androgen levels; restores spontaneous ovulation in many patients | Well-established first-line recommendation in PCOS international guidelines |
| Low glycaemic index (low GI) diet | Reduces insulin spikes; improves hormonal balance | Consistent benefit seen in clinical studies |
| Regular aerobic + strength exercise | Improves insulin sensitivity independently of weight loss | Effective even without significant weight change |
| Metformin | Insulin-sensitising medication; improves ovulation rate and reduces androgen levels | Particularly beneficial in PCOS patients with insulin resistance or elevated fasting glucose |
| Inositol (myo-inositol + D-chiro-inositol) | Improves insulin signalling; shown to improve ovulation and egg quality in PCOS | Growing evidence base; I discuss this with selected patients |
Who this is for: Women with PCOS who are actively trying to conceive and have not yet tried structured lifestyle intervention, or who have mild-to-moderate PCOS with some spontaneous ovulation. Also used as preparation before any fertility treatment to optimise the hormonal environment.
Step 2: Ovulation Induction
When lifestyle intervention alone is insufficient, or when the patient's age or clinical picture makes waiting impractical, ovulation induction is the next step.
Letrozole (Femara)
How It Works
Aromatase inhibitor; temporarily lowers oestrogen, triggering FSH release to stimulate follicle development
First-Line Status
Current international first-line choice for PCOS ovulation induction. A landmark trial showed live birth rates of 27.5% with letrozole versus 19.1% with clomiphene
Clomiphene Citrate (Clomid)
How It Works
Selective oestrogen receptor modulator; stimulates FSH release
First-Line Status
Second-line after letrozole; effective but associated with higher multiple pregnancy rates and thinner uterine lining
Gonadotrophins (FSH injections)
How It Works
Directly stimulate follicle development
First-Line Status
Used when oral agents fail; requires careful monitoring to avoid multiple follicle development and OHSS risk
| Medication | How It Works | First-Line Status |
|---|---|---|
| Letrozole (Femara) | Aromatase inhibitor; temporarily lowers oestrogen, triggering FSH release to stimulate follicle development | Current international first-line choice for PCOS ovulation induction. A landmark trial showed live birth rates of 27.5% with letrozole versus 19.1% with clomiphene |
| Clomiphene Citrate (Clomid) | Selective oestrogen receptor modulator; stimulates FSH release | Second-line after letrozole; effective but associated with higher multiple pregnancy rates and thinner uterine lining |
| Gonadotrophins (FSH injections) | Directly stimulate follicle development | Used when oral agents fail; requires careful monitoring to avoid multiple follicle development and OHSS risk |
Ovulation induction cycles are monitored with serial ultrasounds to confirm follicle development and timing, and to prevent overstimulation. This monitoring is not optional. It is essential.
Who this is for: Women with PCOS who have not responded to lifestyle changes alone, have a partner with acceptable semen parameters, and have open fallopian tubes confirmed on investigation.
Step 3: IUI (Intrauterine Insemination)
IUI is a simple procedure in which washed, prepared sperm are placed directly into the uterine cavity at the time of confirmed ovulation, whether natural or stimulated.
IUI adds value in PCOS when:
- Ovulation induction has produced a mature follicle but natural intercourse timing is uncertain
- Mild male factor is present alongside PCOS
- Up to 3–6 cycles of ovulation induction without pregnancy have occurred
IUI has its limits: if tubes are blocked, if male factor is significant, or if multiple IUI cycles have failed, IVF is the appropriate next step. Repeating IUI beyond 3–4 cycles in the same cycle profile is rarely productive and delays more effective treatment.
Step 4: IVF or IVF with ICSI
IVF is recommended when earlier steps have not resulted in pregnancy, or where the clinical picture makes earlier escalation appropriate. For PCOS specifically, IVF is not a failure. It is often the most logical endpoint of a rational treatment progression.
Why IVF Works Particularly Well for PCOS Patients
PCOS patients often have excellent ovarian reserve, with high antral follicle counts and high AMH levels. This means the ovaries respond well to controlled stimulation and typically produce multiple eggs in a retrieval cycle. In the right hands, this is a significant advantage.
That said, PCOS in IVF requires careful, experienced management. Here is what this means in practice at Ganga Laxmi IVF:
PCOS-Specific IVF Considerations
OHSS Risk (Ovarian Hyperstimulation Syndrome)
Why It Matters in PCOS
PCOS patients have the highest risk of OHSS. Moderate-to-severe OHSS occurs in ~1–5% of all IVF cycles; the risk is significantly higher in PCOS without careful protocol selection
How I Manage It
I use low starting gonadotrophin doses, antagonist protocols, and GnRH agonist trigger in high-risk cases. Where OHSS risk is high, I freeze all embryos and transfer in a separate cycle (freeze-all strategy)
Blastocyst Culture Advantage
Why It Matters in PCOS
PCOS patients often produce many embryos, making blastocyst culture (Day 5) preferable to Day 3 transfer. It identifies the most viable embryos and reduces multiple pregnancy risk
How I Manage It
I recommend blastocyst culture for PCOS patients where embryo numbers permit. Single blastocyst transfer is my standard recommendation
Insulin Resistance and Endometrial Receptivity
Why It Matters in PCOS
Uncontrolled insulin resistance in PCOS can affect uterine lining receptivity, particularly in fresh transfer cycles
How I Manage It
Metformin is continued through stimulation in selected patients. Where the lining is suboptimal after fresh stimulation, frozen transfer in a prepared cycle gives better outcomes
Hyperandrogenism and Egg Quality
Why It Matters in PCOS
Elevated testosterone in poorly controlled PCOS can affect egg quality
How I Manage It
Optimising hormonal parameters before starting IVF, including testosterone levels, is part of my pre-IVF evaluation
Personalised Stimulation Protocol
Why It Matters in PCOS
One stimulation protocol does not fit all PCOS patients. A lean PCOS patient and an obese PCOS patient with insulin resistance have very different risk profiles
How I Manage It
Starting gonadotrophin dose, protocol type, and trigger decision are all individualised based on AMH, antral follicle count, weight, and hormonal profile
| Factor | Why It Matters in PCOS | How I Manage It |
|---|---|---|
| OHSS Risk (Ovarian Hyperstimulation Syndrome) | PCOS patients have the highest risk of OHSS. Moderate-to-severe OHSS occurs in ~1–5% of all IVF cycles; the risk is significantly higher in PCOS without careful protocol selection | I use low starting gonadotrophin doses, antagonist protocols, and GnRH agonist trigger in high-risk cases. Where OHSS risk is high, I freeze all embryos and transfer in a separate cycle (freeze-all strategy) |
| Blastocyst Culture Advantage | PCOS patients often produce many embryos, making blastocyst culture (Day 5) preferable to Day 3 transfer. It identifies the most viable embryos and reduces multiple pregnancy risk | I recommend blastocyst culture for PCOS patients where embryo numbers permit. Single blastocyst transfer is my standard recommendation |
| Insulin Resistance and Endometrial Receptivity | Uncontrolled insulin resistance in PCOS can affect uterine lining receptivity, particularly in fresh transfer cycles | Metformin is continued through stimulation in selected patients. Where the lining is suboptimal after fresh stimulation, frozen transfer in a prepared cycle gives better outcomes |
| Hyperandrogenism and Egg Quality | Elevated testosterone in poorly controlled PCOS can affect egg quality | Optimising hormonal parameters before starting IVF, including testosterone levels, is part of my pre-IVF evaluation |
| Personalised Stimulation Protocol | One stimulation protocol does not fit all PCOS patients. A lean PCOS patient and an obese PCOS patient with insulin resistance have very different risk profiles | Starting gonadotrophin dose, protocol type, and trigger decision are all individualised based on AMH, antral follicle count, weight, and hormonal profile |
Why freeze-all matters in PCOS IVF
In PCOS patients at higher OHSS risk, I frequently recommend freezing all embryos after retrieval and transferring in a separate hormonal cycle. This approach eliminates fresh transfer OHSS risk entirely and allows the uterine environment to normalise before implantation. The pregnancy rates with frozen-thawed transfer in PCOS are equivalent to, and in some studies better than, fresh transfer.
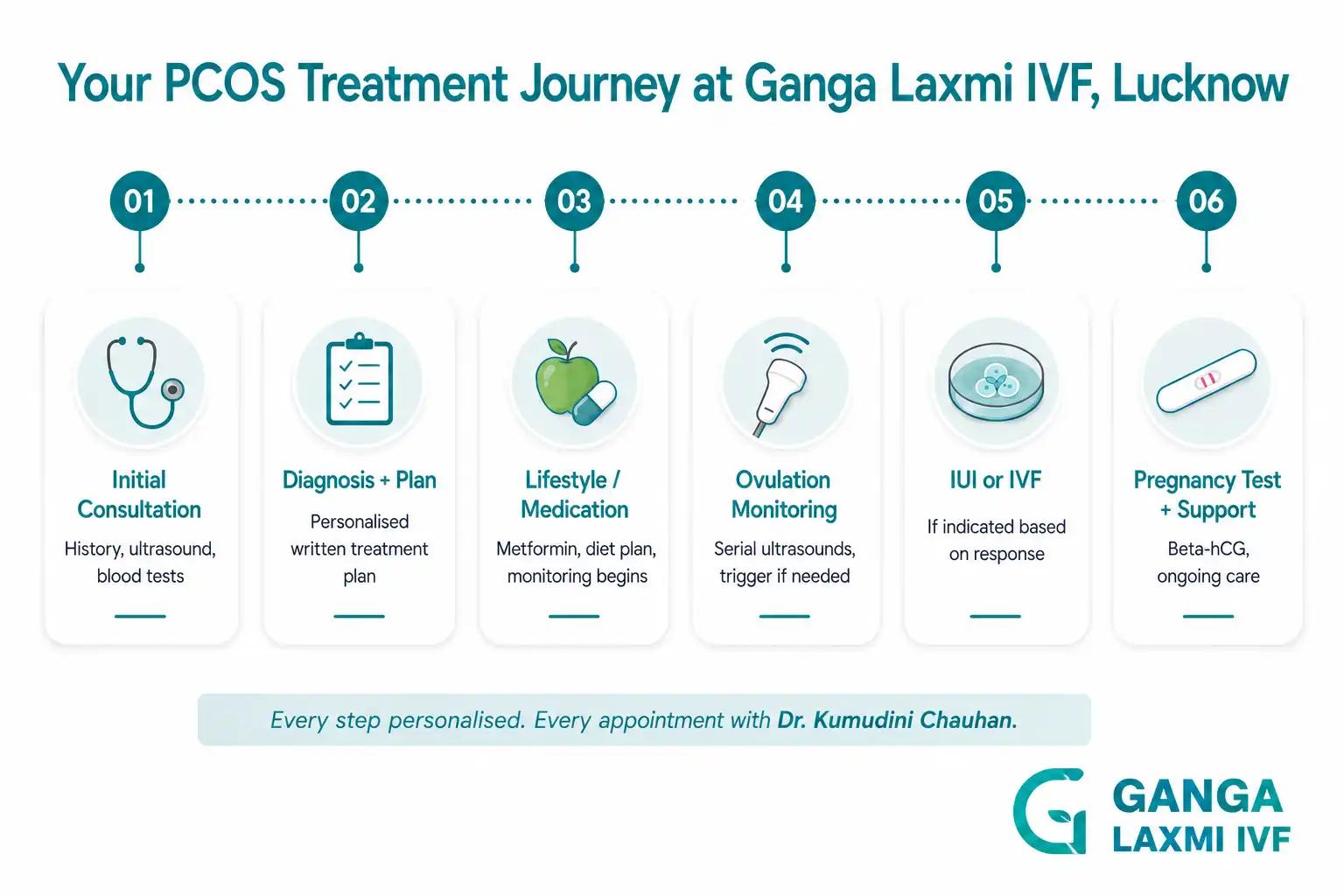
What to Expect at Ganga Laxmi IVF if You Have PCOS
Every PCOS patient who comes to me receives a complete clinical evaluation, not a template. PCOS presents differently in every woman, and the treatment plan must reflect that.
Your PCOS Consultation at Ganga Laxmi IVF
What I assess at the first visit:
- Detailed menstrual history covering cycle length, regularity, and any prior ovulation confirmed or denied
- Prior fertility investigations and treatments
- Weight, BMI, and clinical signs of insulin resistance or hyperandrogenism
- Transvaginal ultrasound covering antral follicle count, ovarian morphology, and uterine assessment
- Blood tests on the appropriate cycle day: FSH, LH, AMH, testosterone, prolactin, TSH, fasting insulin and glucose, Vitamin D
- Partner's semen analysis, because PCOS does not exist in isolation and I evaluate both partners at the outset
What comes out of that consultation: a clear, written treatment recommendation with the rationale explained, not a generic protocol and not a rushed decision. I explain exactly why I am recommending what I am recommending, what the alternatives are, and what realistic success looks like for your specific profile.
AMH and antral follicle count
Why It Matters
Confirms PCOS, quantifies ovarian reserve, guides IVF dose selection
Fasting insulin and glucose
Why It Matters
Identifies insulin resistance, which directly changes medication decisions
Thyroid function (TSH)
Why It Matters
Thyroid disorders are significantly more common in PCOS women; uncontrolled hypothyroidism directly impairs IVF success
Testosterone and prolactin
Why It Matters
Rules out other hormonal causes; guides ovulation induction choice
Transvaginal ultrasound
Why It Matters
Checks for fibroids, polyps, or other uterine factors that need addressing before treatment
Semen analysis
Why It Matters
Male factor is present in ~40–50% of couples presenting with infertility; PCOS does not exclude male factor
| Consultation Item | Why It Matters |
|---|---|
| AMH and antral follicle count | Confirms PCOS, quantifies ovarian reserve, guides IVF dose selection |
| Fasting insulin and glucose | Identifies insulin resistance, which directly changes medication decisions |
| Thyroid function (TSH) | Thyroid disorders are significantly more common in PCOS women; uncontrolled hypothyroidism directly impairs IVF success |
| Testosterone and prolactin | Rules out other hormonal causes; guides ovulation induction choice |
| Transvaginal ultrasound | Checks for fibroids, polyps, or other uterine factors that need addressing before treatment |
| Semen analysis | Male factor is present in ~40–50% of couples presenting with infertility; PCOS does not exclude male factor |
Ganga Laxmi IVF is located in Gomti Nagar, Lucknow, and unlike large chain fertility clinics, you will see me at every significant appointment. I do not outsource the interpretation of your investigations or the planning of your treatment to a junior team member.
A Patient's Journey: PCOS and IVF at Ganga Laxmi IVF
Name and identifying details changed with patient consent.
Priya was 29 years old when she first came to see me. She had been trying to conceive for almost three years. Her periods had always been irregular, sometimes arriving every 45 to 60 days, sometimes skipping entirely, but she had been told this was “just her body.” No investigation had been done. No ovulation had ever been confirmed.
Her husband's semen analysis was normal. An ultrasound at our first visit showed classic polycystic ovarian morphology bilaterally, and her AMH came back significantly elevated. Her testosterone was mildly raised and her fasting insulin suggested moderate insulin resistance.
We started with metformin and a structured low-GI dietary plan, alongside monitoring. Three months later, there was some improvement in cycle regularity but no confirmed ovulation. We moved to letrozole with monitoring. Two cycles, follicles developing but not triggering spontaneously. We added an HCG trigger injection on the third letrozole cycle. Her follicle matured, ovulation was confirmed, and she did not conceive.
After one IUI cycle that also did not result in pregnancy, Priya and I sat down for an honest conversation. She was 30 by this point, her parameters were good, and I felt her best chance lay in IVF. We planned a freeze-all cycle given her high AFC and OHSS risk. Stimulation went smoothly with a low-dose antagonist protocol. She produced 14 eggs, 11 were mature, 9 fertilised normally. Five developed to blastocyst stage. We froze all five.
In her first frozen embryo transfer two months later, a single blastocyst was transferred. Fourteen days after transfer, her beta-hCG was positive. She delivered a healthy baby girl eight months later.
Three years of uncertainty, and an 18-month treatment journey that moved deliberately through each appropriate step. Priya's outcome is not unusual for PCOS. In my experience, it is what happens when the right treatment is given in the right sequence.
Help centre
Frequently Asked Questions
These are the questions I hear every week from PCOS patients, including questions people hesitate to ask but absolutely should.
PCOS itself does not necessarily worsen with age. In fact, many women with PCOS find that their cycles become slightly more regular in their late thirties as AMH levels naturally begin to decline and the ovarian reserve shrinks. Paradoxically, this can sometimes improve spontaneous ovulation. However, fertility does decline with age regardless of PCOS, and ovarian reserve is finite. A woman with PCOS at 34 has meaningfully fewer eggs and a lower probability of successful IVF per cycle than she did at 28. This is the single most important reason I encourage PCOS patients not to delay evaluation. PCOS does not protect you from age-related fertility decline; it simply adds a separate, treatable layer to the challenge.
IVF is not the only option, and I do not recommend it to every PCOS patient. Many women with PCOS conceive with ovulation induction using letrozole or clomiphene, particularly younger patients with no additional fertility factors and partners with normal semen parameters. The treatment ladder exists for a reason: lifestyle, then ovulation induction, then IUI, then IVF. I move a patient along this ladder based on clinical response, age, and time, not on a fixed schedule. What I try to avoid is keeping a patient on a treatment that is clearly not working because it is "less invasive." Appropriate escalation at the right time is the kindest thing I can do clinically.
PCOS is diagnosed using the Rotterdam Criteria. You need at least two of the following three features: 1) Irregular or absent ovulation, meaning cycles consistently longer than 35 days, or fewer than 8 periods per year. 2) Clinical or biochemical signs of excess androgens such as acne (particularly jawline), hirsutism (excess facial/body hair), or elevated testosterone on blood test. 3) Polycystic ovarian morphology on ultrasound showing 20 or more small follicles per ovary, or ovarian volume greater than 10 mL. Do not ignore: periods that come every 45, 60, or 90 days (or not at all); darkened skin around your neck or armpits, which is a sign of insulin resistance; unexplained difficulty conceiving when everything else appears normal; a family history of PCOS, type 2 diabetes, or early cardiovascular disease. A correct diagnosis requires both a blood test (ideally on Day 2–5 of a natural cycle, or at any time if cycles are absent) and a transvaginal ultrasound. Neither test alone is sufficient.
This is a question I take very seriously, because the research is nuanced and patients deserve an honest answer. PCOS is associated with a moderately elevated risk of miscarriage compared to women without PCOS. Studies suggest the early miscarriage rate in PCOS is approximately 20 to 35 percent, versus 10 to 15 percent in the general population. The elevated risk is linked primarily to insulin resistance and elevated androgens, both of which can affect early embryo development and uterine receptivity. Importantly, this risk is modifiable. Optimising insulin sensitivity before and during treatment (with metformin, dietary changes, and normalising testosterone levels) reduces miscarriage risk. In IVF, transferring a blastocyst rather than a Day 3 embryo selects for embryos that have already demonstrated developmental competence, and this reduces the proportion of genetically abnormal embryos being transferred. I do not share this information to alarm patients. I share it because patients who know their risk factors can take meaningful steps to reduce them, and that is exactly what we do together at Ganga Laxmi IVF.
Here is exactly what I assess at your first visit: Day 2–3 FSH, LH, and Oestradiol for baseline hormonal profile; AMH to confirm high ovarian reserve typical of PCOS and guide IVF dosing; Testosterone (total and free) to confirm hyperandrogenism; Prolactin to exclude elevated prolactin which mimics PCOS; TSH for thyroid function as thyroid disorders co-exist with PCOS frequently; Fasting insulin and fasting glucose (HOMA-IR) to quantify insulin resistance; Vitamin D, as deficiency is very common in PCOS in Uttar Pradesh; Transvaginal ultrasound to confirm polycystic ovarian morphology, antral follicle count, and assess uterine cavity; and your partner's semen analysis, because male factor is present in approximately 40 to 50 percent of infertile couples. First consultation fee is Rs. 400. You will leave with a clear picture of what is causing the difficulty and a structured plan for what comes next.
Yes. The absence of a regular period means ovulation is not occurring on its own, but ovulation can be induced medically. Some of the most straightforward PCOS fertility cases I treat are women with very long, irregular cycles whose ovaries respond excellently to letrozole or IVF stimulation, because their ovarian reserve is strong and the only problem is the absence of a trigger to ovulate. What irregular cycles tell me clinically is that natural timed intercourse is ineffective and that monitored ovulation induction is the right starting point. It does not tell me that pregnancy is impossible. Far from it.
You Have More Options Than You Think
PCOS is the most common cause of anovulatory infertility in India, and it is also the most treatable. Women with PCOS who receive accurate diagnosis, appropriate treatment in the right sequence, and consistent follow-up have excellent outcomes across every stage of the treatment ladder, from letrozole to IVF.
If you have been trying to conceive, if your cycles are irregular, or if you have been told you have PCOS and want to understand your fertility options clearly, I would like to meet you.
PCOS fertility consultation
Book a PCOS fertility consultation
Irregular cycles, no ovulation, or unsure which treatment step is right for you. Get a personalised PCOS assessment with Dr. Chauhan at Ganga Laxmi IVF, Gomti Nagar.
- Clinic
- 2/301, J N Singh Marg, Viram Khand-2, Gomti Nagar, Lucknow, 226010
- Hours
- Monday to Saturday, 9:00 AM to 8:00 PM
- Phone
- +91 72756 49692
- First consultation
- From Rs. 400
About the author
Dr. Kumudini Chauhan
Dr. Kumudini Chauhan
PCOS & fertility
Dr. Chauhan is a senior gynaecologist and infertility specialist in Gomti Nagar, Lucknow with over 20 years of experience. She is dedicated to providing honest, evidence-based guidance to couples navigating fertility challenges.
Keep reading
Related articles

Kangaroo Mother Care (KMC): A Simple Yet Powerful Way to Save Newborn Lives
What is Kangaroo Mother Care? Learn how skin-to-skin contact saves premature babies, improves breastfeeding, and supports growth. A complete KMC guide.

IVF After a Failed Cycle: What to Do Next, and Why It Still Works
A failed IVF cycle does not mean the end. Dr. Kumudini Chauhan, Lucknow, explains what causes failure, what changes for the next cycle, and why many patients succeed after one setback.
Male Infertility Treatment in Lucknow: Causes, Tests & Complete Guide
Male factors contribute to roughly half of all infertility cases. Dr. Kumudini Chauhan explains what causes male infertility, what a proper investigation looks like, and which treatments, from lifestyle changes to ICSI, are available at Ganga Laxmi IVF, Lucknow.

Laser Hatching and PGT After Failed IVF: Why Your Previous Cycles Failed and What to Do Next
Dr. Kumudini Chauhan explains why IVF fails, how Laser Assisted Hatching and PGT address those specific causes, and what a proper failed-IVF workup looks like at Ganga Laxmi IVF.